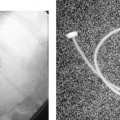
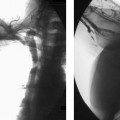
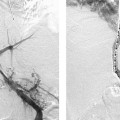
CASE 4 An 83-year-old male presented to the emergency room of an outside hospital complaining of new-onset, right-sided epigastric pain and emesis after a fall. He had a history of resection of the left lobe of the liver for hepatocellular carcinoma 3 years earlier and a 40-pound weight loss over the last 6 months. Physical examination revealed pallor, tachypnea, diaphoresis, and right upper-quadrant tenderness. Hemoglobin was 7.9 g/dL. The patient was stabilized with blood products and fluids and was transferred for further treatment. Figure 4-1 Contrast-enhanced CT of the abdomen shows active contrast extravasation, massive hemoperitoneum, and a ruptured, heterogeneous, enhancing mass within the right lobe of the liver. Contrast-enhanced CT showed a ruptured enhancing mass involving the right lobe of the liver with actively extravasating contrast material and massive hemoperitoneum (Fig. 4-1). Post-traumatic laceration of hepatocellular carcinoma. Upon completion of the CT, the patient was moved to the angiography suite. Celiac angiography was performed from the femoral approach using a 5-French (F) visceral selective catheter (RC-1, Boston Scientific, Natick, Massachusetts). There was marked enhancement of the liver mass in the right lobe and arteriovenous shunting (Fig. 4-2A). A 3F catheter was used to selectively catheterize and embolize the involved intrahepatic arterial branches using a slurry of Gelfoam (Pharmacia and Upjohn, Kalamazoo, Michigan) particles. Successful embolization of the tumor was verified by selected hepatic arteriography (Fig. 4-2B). After the procedure, the patient’s hemodynamic status stabilized, and his hemoglobin level stabilized above 12.0. He was discharged from the hospital 4 days after embolization with plans to follow up with his primary physician for treatment of recurrent hepatocellular carcinoma. Figure 4-2 (A
Clinical Presentation

Radiologic Studies
Diagnosis
Treatment

![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


