40 Incidental Pelvic Mass
40.1 Case Presentation
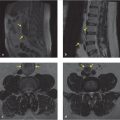
A 39-year-old woman presented with lower back pain for which an MRI of the lumbar spine without intravenous (IV) contrast was performed (▶ Fig. 40.1).

40.2 Imaging Findings and Impression
The MRI images demonstrate an incidentally detected, partially visualized multilocular cystic left adnexal mass with slightly thickened septations (arrows in ▶ Fig. 40.1). The abnormality is at the edge of the field of view and incompletely characterized on this examination. Benign physiologic ovarian/corpus luteal cysts are the most common cystic lesions in young, premenopausal women. In this case, however, the size and presence of septations warrant further workup and complete imaging.
40.2.1 Additional Testing Needed
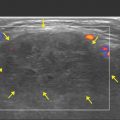
A pelvic ultrasound with transabdominal and transvaginal imaging is the first modality to work up a uterine or adnexal lesion (▶ Fig. 40.2).
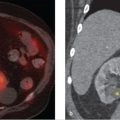
Cross-sectional imaging with CT and/or MRI with contrast can also be utilized in more complex cases and for problem-solving if ultrasound is inconclusive.

40.2.2 Pelvic Ultrasound Findings and Impression
Pelvic ultrasound examination done approximately 12 weeks later demonstrates a 9-cm large multilocular cystic mass with thickened septations. No internal vascularity is demonstrated. Findings are concerning for cystic ovarian neoplasm; therefore, referral to gynecologist was made. Due to size (> 7 cm), persistence on follow-up imaging, and internal complexity, the lesion was excised.
Follow-up: The patient underwent a left oophorectomy and final pathology revealed a serous cystadenoma.
40.3 Essential Information regarding Ovarian Serous Cystadenomas
Ovarian serous cystadenoma is a benign lesion classified as epithelial ovarian neoplasm and often indistinguishable from functional ovarian cysts on imaging.
It can be encountered at any age, but peak incidence is typically in the fourth and fifth decades of life.
It accounts for 25% of all benign ovarian neoplasms and 10 to 20% are bilateral.
Key in distinguishing it from a physiologic ovarian cyst is its size (average of 10 cm) and persistence on follow-up examinations (most important differentiating factor).
It can be multilocular with septations, but will usually not have internal vascularity within the septation or solid component such as mural nodules. The best initial imaging tool for characterization is ultrasound (▶ Table 40.1).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


