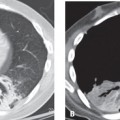
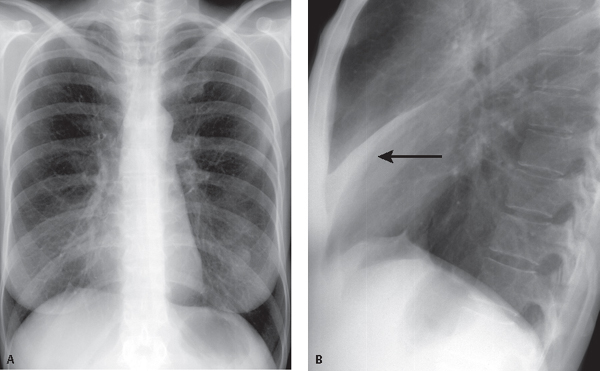
CASE 40 68-year-old man with a long history of tobacco abuse experiencing a recent change in the nature of his pre-existing chronic “smoker’s” cough PA (Fig. 40.1A) chest radiograph reveals an ill-defined right perihilar opacity that partially obscures the right heart border and contains no air bronchograms. On the coned-down lateral radiograph (Fig. 40.1B), there is a corresponding triangular opacity with its base abutting the sternum and its apex directed toward the hilum. Note the anterior displacement of the oblique fissure (arrow) and elevation of the right hemidiaphragm. Right Middle Lobe Atelectasis; Occult Endobronchial Squamous Cell Cancer • Uncomplicated Right Middle Lobe Atelectasis (e.g., mucus plug) • Complicated Right Middle Lobe Atelectasis from Other Primary or Secondary Endobronchial Neoplasms • Right Middle Lobe Syndrome • Right Middle Lobe Pneumonia Fig. 40.1 Right middle lobe atelectasis is one of the easiest diagnoses to make on lateral chest radiography (Figs. 40.1B, 40.2B) but one of the most difficult on frontal chest exams (Figs. 40.1A, 40.2A). As the middle lobe loses volume, the horizontal fissure and the lower half of the oblique fissure approximate, forming a “triangular” opacity with its apex at the hilum and its base against the parietal pleura behind the sternum. These fissures almost contact one another, with complete lobar collapse manifesting as a thin, almost imperceptible retrosternal triangular opacity (Fig. 40.3). On frontal exams, there may be no obvious increase in radio-opacity. The only radiologic sign of middle lobe volume loss may be a partial silhouette of the right heart border due to the contiguity of the medial segment of the middle lobe with the right atrium (Figs. 40.1A, 40.4A). Air bronchograms are a reliable sign that a process is parenchymal. The most common causes are pneumonia and pulmonary edema. Air bronchograms may also be seen in atelectatic lobes if the airway is patent. Compensatory indirect
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine