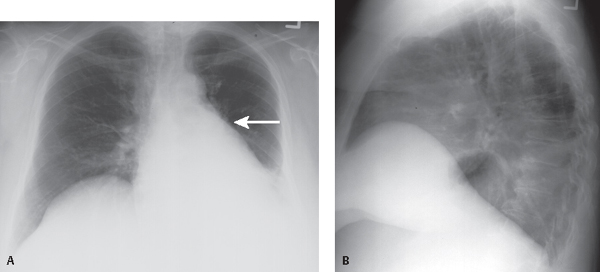
CASE 43 65-year-old woman with a long history of tobacco abuse has developed intermittent hemoptysis and progressive cough PA (Fig. 43.1A) and lateral (Fig. 43.1B) chest exams reveal a relatively small left thorax, leftward mediastinal shift, and increased opacity in the lower left lung silhouetting the diaphragm. A localized basilar opacity overlies the lower thoracic spine (positive spine sign) and silhouettes the posterior-lateral diaphragm. There is loss of definition of the left hilum and the interlobar pulmonary artery is inconspicuous. Note the focal convexity in the medial aspect of the displaced oblique fissure (reverse “S” sign of Golden) (arrow) indicating the presence of an obstructing central hilar mass. Left Lower Lobe Atelectasis; Obstructing Small Cell Lung Cancer • Post-Obstructive Lower Lobe Atelectasis from an Endobronchial Mass (e.g., primary and secondary neoplasia) • Post-Obstructive Lower Lobe Atelectasis from Extrinsic Bronchial Compression by Reactive or Neoplastic Lymphadenopathy Fig. 43.1 The right and left lower lobes demonstrate similar patterns of lobar collapse on imaging. The triangular versus rounded configuration assumed by the atelectatic lower lobe is related to the fulcrum-like effect exerted on the lung by the hilum and the integrity of the pulmonary ligament. When the pulmonary ligament is complete, the lower lobe is tethered to the mediastinum and hemidiaphragm and maintains a close relationship to both structures, assuming a triangular configuration as it loses volume (Figs. 43.2, 43.3). Alternatively, when the pulmonary ligament is incomplete, the lung base is not adherent to the diaphragm. When the lower lobe loses volume, its shape depends primarily on its mediastinal attachment and the collapsed lobe assumes a more rounded morphology, often creating an apparent left-sided paraspinal mass (pseudomass sign). As the left lower lobe loses volume, the cephalad and caudal aspects of the oblique fissure shift backward and downward, approximating one another. This is best appreciated on lateral chest studies (Fig. 43.4). With increased volume loss, the atelectatic lobe may silhouette the posterior diaphragm, adding to the density of the lower thoracic spine (positive spine sign
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


