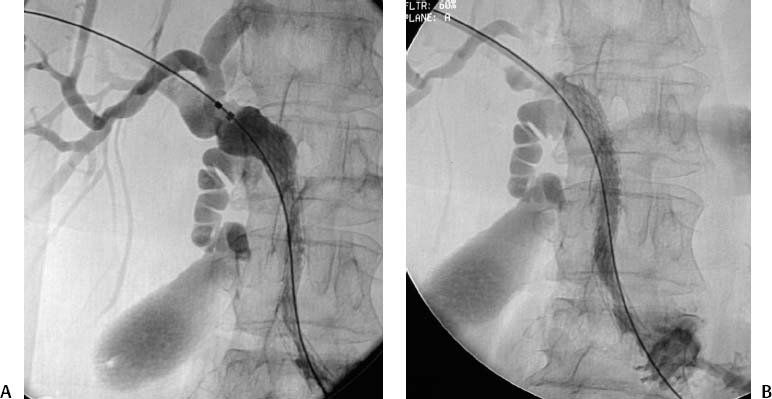
CASE 43 A 65-year-old male with a history of biopsy-proven pancreatic carcinoma was admitted to the medicine service with nausea, fever, and jaundice. He had elevated serum bilirubin and alkaline phosphatase levels and was referred to interventional radiology for biliary decompression. Figure 43-1 A 65-year-old male with a history of biopsy-proven pancreatic carcinoma. (A) Percutaneous cholangiogram shows marked dilatation of the main right intrahepatic bile duct and no opacification of the extrahepatic or left intrahepatic bile ducts. An internal-external biliary drain was placed. (B) Repeat cholangiogram after a period of biliary drainage reveals markedly dilated right and left intrahepatic ducts and diffuse stenosis of the extrahepatic ducts delaying spillage of contrast material into the small bowel. Percutaneous cholangiography showed marked dilatation of the main right intrahepatic bile duct and no opacification of the extrahepatic or left intrahepatic bile ducts (Fig. 43-1A). After a period of internal-external biliary drainage, cholangiography revealed markedly dilated right and left intra-hepatic ducts and diffuse stenosis of the extrahepatic ducts delaying spillage of contrast material into the small bowel (Fig. 43-1B). Malignant biliary obstruction resulting from pancreatic carcinoma. From the right peripheral bile duct, access was achieved across the stenotic extrahepatic bile duct using a stiff Amplatz wire (Cook, Bloomington, Indiana). A 7-French (F) sidearm sheath was advanced and a 10-mm diameter, 8-cm long Wallstent (Boston Scientific, Natick, Massachusetts) was deployed with the caudal end in the duodenum and the cranial end in the right main intrahepatic duct (Fig. 43-2). Further dilatation was performed with a BlueMax balloon catheter (8 mm diameter; Boston Scientific, Natick, Massachusetts). Contrast injection through the sidearm sheath demonstrated free flow from the right intrahepatic ducts to the duodenum. The external access was removed. The patient succumbed to complications of metastatic disease 154 days after stent placement, without recurrence of symptomatic biliary obstruction. 0.035″ Amplatz wire (Boston Scientific, Natick, Massachusetts) 7F vascular sheath (Cook, Bloomington, Indiana) 10- × 80-mm self-expanding stent 8-mm diameter BlueMax balloon catheter (Boston Scientific, Natick, Massachusetts)
Clinical Presentation

Radiologic Studies
Diagnosis
Treatment
Equipment
Discussion
Background
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


