44 Bone Tumors
Primary and secondary bone tumors in the hand are rare. The fact that the most common bone tumors of the hand have a relatively characteristic radiographic morphology facilitates differential diagnosis. However, the entire spectrum of bone tumors, including tumorlike lesions, can appear in the hand. Lesions in atypical locations, such as the carpal bones, often require a biopsy for diagnosis. Radiographs provide essential information for the classification of these tumors. MRI delivers important additional information in some tumorous entities. It is the method of choice to determine the extent of the tumor for planning therapy. CT imaging is useful in searching for the nidus of an osteoid osteoma and, to a certain extent, in osteosclerotic tumors. Skeletal scintigraphy is applied for the evaluation of osteoid osteomas, polyostotic neoplastic disease, and, in individual cases, differentiation from osteomyelitis.
Pathoanatomy and Clinical Symptoms
Tumors of the hand are mostly soft-tissue tumors. Bone tumors of the hand constitute only 2% in overall statistics from centers for hand surgery. Data from bone-tumor centers show that of all bone tumors, only 4% are located on the skeleton of the hand. One reason for this is the very early conversion of the bone marrow of the hand into fatty marrow. Primary tumors associated with hematopoietic marrow and metastases are generally located at or near the trunk. Other tumors and tumorlike lesions develop on skeletal parts with high longitudinal growth and metaphyseal remodeling, such as those around the knee joint.
The distribution of the benign/malignant nature of bone tumors of the hand is remarkable ( Table 44.1 ). Centers for hand surgery report that 97% of their patients’ tumors are benign. Even in the preselected patient population in these centers, the proportion of benign lesions among bone tumors of the hand is 90%. Malignant bone tumors in the hand are thus extremely rare. A further peculiarity is that soft-tissue tumors in the hand lead to secondary skeletal changes earlier than in other parts of the body because of their close proximity to bones and the limited spaces in the hand in which they can expand.
Diagnostic Imaging
Radiography
Conventional radiographs of the hand are fundamental for assessment in all tumor cases. Documentation of osteoblastic and osteolytic bone changes destruction of cortical and cancellous bone serve as diagnostic criteria. Periosteal reaction and involvement of the paraosseous soft tissues provide information about the speed of growth and the nature of the tumor. Assessment of the tumor matrix often makes it possible to determine the tumor entity. A few tumorous lesions have multicentric manifestations on the hand.
Arteriography
The diagnostic value of arteriography in the evaluation of bone tumors is very limited. Aside from rare exceptions, imaging of the vasculature is only indicated for surgical planning with large tumors.
Nuclear Medicine
Skeletal scintigraphy has only secondary importance in the evaluation of bone tumors in the hand. Its most important contribution is identification of an osteoid osteoma, as the nidus can occasionally escape detection in survey radiographs. This is often the case particularly in the carpal area.
Computed Tomography
MRI has replaced CT in assessment of soft tissues for planning surgery. An important indication for CT imaging, however, is the clinical or scintigraphic suspicion of an osteoid osteoma. The multiplanar capability provided by spiral CT extends its spectrum of indications to periarticular cystic osteolyses and osteosclerosing tumors. Cortical destruction of the carpal bones can also be identified reliably.
Magnetic Resonance Imaging
The most important and comprehensive information about the osseous hand skeleton and surrounding soft tissues for surgical planning is provided by MRI. Multiplanar imaging with the use of surface coils when malignancy is suspected provides the most reliable information about the size of the tumor and its relation to surrounding soft tissues. It is important to obtain as much information as possible about tumor spread into the medullary space of bones. MRI is particularly useful for evaluation of enchondromas, which are the most common bone tumors in the hand, since these tumors display a characteristically high-signal intensity in T2-weighted sequences. Although small pathologic tumor vessels cannot be visualized, integration of MR angiography into the MRI sequence protocol allows determination of the tumor location in relation to blood vessels and the frequent vascular variants.
Tumor Entities
Bone Tumors of Chondrogenous Origin
Enchondroma (Chondroma)
Pathoanatomy and Clinical Symptoms
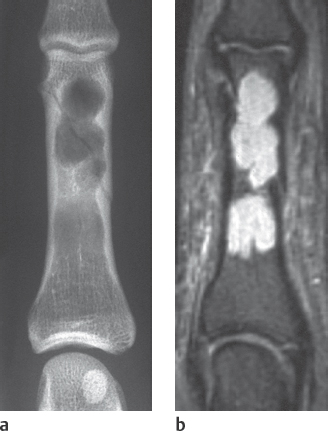
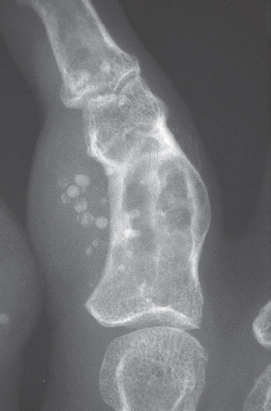
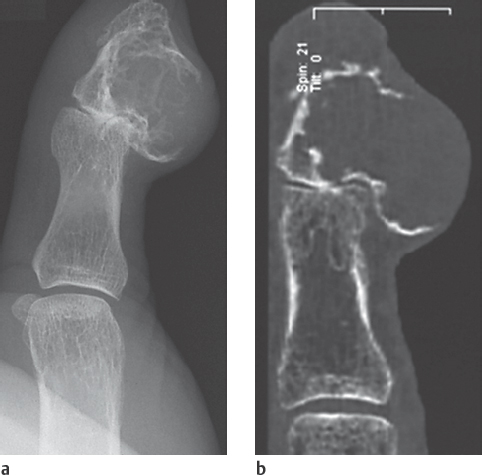
Enchondromas are the most common bone tumor of the hand skeleton. They consist of mature cartilaginous cells, which presumably develop from displaced epiphyseal cartilage. For this reason, they are most often found in the distal parts of the metacarpals and in the proximal parts of the phalanges. They show little growth potential. An enchondroma is usually a coincidental finding or is detected with pathologic fractures (Fig. 44.1 a), generally between the second and fifth decades of life. There is no sex predisposition. Aside from an occasional slight distension of the affected bone, it causes no complaints. In contrast to histologically similar lesions of the long tubular bones, enchondromas have only a very slight tendency to become malignant. This is not true for enchondromatosis, which is a special polyostotic form with possible malignant transformation in up to 30% of cases. The purely polyostotic form (Ollier disease) is differentiated from Maffucci syndrome ( Fig. 44.3 ), which is a combination of multiple enchondromas and soft-tissue hemangiomas.
Diagnostic Imaging
Radiography
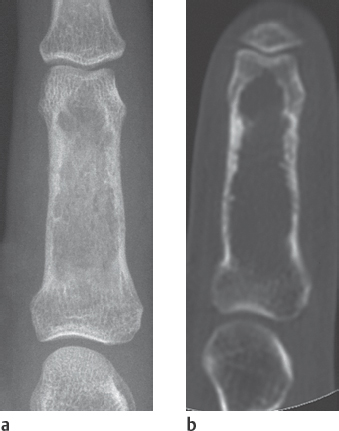
The radiographic appearance is characterized by a sharply contoured osteolysis with endosteal bone resorption in the phalanges and metacarpal bones ( Figs. 44.1 , 44.2 ). The carpal bones are almost never affected. A thin osteosclerotic margin and a moderate, blistery distension are common. Periosteal reactions are rarely seen and usually result from reparative healing processes following pathologic fractures. Identification of punctate calcifications within the cartilaginous matrix of the tumor, which resemble popcorn, are strongly pathognomonic for this tumor entity. A special form with the same tumor characteristics is the periosteal chondroma ( Figs. 44.4 , 44.5 ).
Magnetic Resonance Imaging
The cartilaginous tumor matrix has a characteristic lobulated appearance, expansive tumor growth, and high signal intensity in T2-weighted MRI sequences. Differentiation from a low-grade chondrosarcoma, which is difficult to perform in the long tubular bones, is of secondary importance in the skeleton of the hand.
Differential Diagnosis
Solitary bone cysts, aneurysmal bone cysts, epidermoid cysts, giant-cell tumors, chondrosarcomas, and other rare bone tumors must also be considered.

Osteochondroma (Cartilaginous Exostosis)
Pathoanatomy and Clinical Symptoms
Osteochondromas of the hand, which are benign lesions of cartilaginous origin, are considerably rarer than enchondromas and are also often detected only incidentally. Their development is associated with the epiphyseal plates, and they often appear as hereditary multiple exostoses in familial exostosis disease. Osteo-chondromas are frequently accompanied by growth disturbance.
Diagnostic Imaging
Radiography
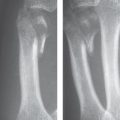
The radiographic finding with cone-shaped or cauliflower-shaped protrusions is characteristic ( Figs. 44.6 , 44.7 ). A special carpal form is exostosis in Trevor disease (dysplasia epiphysealis hemimelica), which can also be manifested as an articular chondroma.
Magnetic Resonance Imaging
The nonossified cartilaginous caps on the exostoses can only be seen with MRI. The cartilaginous caps appear hyperintense in T1- and T2-weighted sequences ( Fig. 44.8 ). Their malignant transformation into chondrosarcoma can be detected more reliably with MRI than with radiographic procedures.
Differential Diagnosis
Carpal bossing (carpe bossu) (see Fig. 28.1 ), an exostotic protrusion on the back of the hand, is considered an os styloideum, and thus a normal variant and not a tumor. Chronic mechanical irritation can lead to exostotic protuberances on the short tubular bones of the hand as a result of new periosteal bone formation. Ossification of a periosteal hematoma on the diaphyses of the short tubular bones is considered responsible for Turret exostosis ( Fig. 44.9 ). Subungual exostosis is also a reactive form of bone transformation.




Chondroblastoma, Chondromyxoid Fibroma
Both benign tumor entities are very rare and have only been observed on the hand in individual cases. The chondroblastoma differs from the enchondroma in its predisposed epimetaphyseal location. Marginal osteosclerosis and periosteal reactions are often seen in chondromyxoid fibromas.
Chondrosarcoma
Pathoanatomy and Clinical Symptoms
Chondrosarcomas are by far the most common of the extremely rare primary bone malignancies of the hand. The proportion of secondary chondrosarcomas is about 20%. These usually develop from Ollier disease or Maffucci syndrome. Males are somewhat more often affected, but there is no predisposed age.
Diagnostic Imaging
Radiography
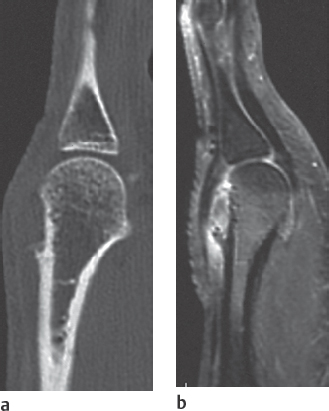
The sites most often affected are the metacarpals and the proximal phalanges. In comparison to enchondromas, chondrosarcomas cause destruction of the cortical bone and formation of extraosseous soft tissue. Enchondral calcifications facilitate the classification of this tumor ( Fig. 44.10 ).
Computed Tomography
The expansive osteolytic lesions caused by chondrosarcomas lead to early focal destruction of the periosteum on the hand skeleton, which is best visualized with CT. The sensitivity in confirming endotumorous calcifications is higher in CT than in radiography.
Magnetic Resonance Imaging
The cartilaginous tumor matrix has a characteristic appearance in MRI similar to that of enchondromas, with marked high-signal intensity in T2-weighted sequences. The criteria of malignancy, i.e., penetration of the cortical bone and extraosseous tumor spread, also indicate the tumor entity. Dynamic MRI displays a more rapid contrast enhancement behavior than is seen in enchondromas.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


