45 Soft-tissue Tumors
On the hand, soft-tissue tumors are more common than bone tumors. If the results of clinical examination remain equivocal, the localization and size of the tumor can be precisely determined with imaging methods. High-resolution ultrasonography (US) allows identification of the commonly occurring ganglion cysts, as well as their sites of origin. For all tumors of the hand, contrast-enhanced MRI is the method of choice for further investigation. It provides exact information regarding the localization and type of tissue of the tumor. Specific patterns are seen in ganglion cysts, epidermal inclusion cysts, lipomas, hemangiomas, giant-cell tumors of the tendon sheaths, glomus tumors, and tumors of the nerve sheaths. When a malignant soft-tissue tumor is suspected, the exact tumor extent should be determined before biopsy or surgical excision is undertaken.
Pathoanatomy and Clinical Symptoms
In contrast to the WHO pathoanatomic definition, the soft tissues will be summarized from a radiodiagnostic viewpoint as those tissues that do not originate from bones or joints. In principle, all soft-tissue tumors can be manifested in the hands and are more common than bone tumors. Some entities occur at predisposed sites on the hand. The tumors are usually benign (about 15 % of all benign tumors), with ganglion cysts making up about 60%. Malignant soft-tissue tumors of the hand are rare (about 4% of all malignomas). Superficial tumors on the hand are noticed early by patients or their companions. These tumors are generally of epithelial origin and can often be clinically classified without additional technical examinations. Space-occupying lesions that are located deeper in the hand lead to functional impairment earlier and also to pain because of the high density of the neural network in the hand. However, there are often only uncharacteristic symptoms such as swelling, discomfort, and pain, or an ambiguous finding on clinical examination.
Diagnostic Imaging
Radiography
Although most of the diagnostic parameters listed in Table 45.1 cannot be evaluated with conventional radiographs, survey radiographs in two planes should be performed when a soft-tissue tumor is suspected for the following reasons:
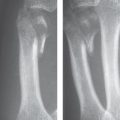
Exclusion of a skeletal deformity, such as an exostosis (see Figs. 44.6 – 44.9 ), carpal bossing (see Fig. 28.1 ), or a hypertrophic callus, as the cause of the tumor.
Exclusion of a secondary osseous reaction. A soft-tissue tumor can induce a periosteal reaction in the neighboring bones, bone deformity with smoothly contoured, osteosclerotic margins as a result of remodeling or scalloping (see Fig. 44.15 ), or bone destruction (see Fig. 44.24 ).
Identification of calcifications in soft tissues, which can provide diagnostic evidence of, e.g., a hemangioma when phleboliths are present (see Fig. 44.3 ) and myositis ossificans when a dense, peripheral pattern of calcification is seen.
Ultrasonography
In the search for clinically occult ganglion cysts and tissue characterization of palpable soft-tissue lesions, US examination should be performed first. Prerequisites are the application of a high-frequency probe (optimally 10–14 MHz) and an examiner with much experience in ultrasonic diagnosis of abnormalities of the hand. An advantage of US is the possibility of obtaining real-time, multiplanar scans. Disadvantages are the inadequate determination of the extent of the tumor because of bone-related shadowing if the tumor is located deep in the hand, and the often unspecific echo pattern of the tumor. Only anechoic ganglion cysts have a characteristic echo texture. In many cases, however, even the entity of neural tumors, lipomas, and vascular tumors can be determined by their echo characteristics. US makes it possible to guide a puncture real-time from the soft-tissue lesion.
Computed Tomography
CT is not very valuable in evaluation of the soft tissues of the hand because the absorption differences between the tumor and uninvolved soft tissues or the edema surrounding the tumor almost always provide too little contrast in comparison to the differences in signal intensity in MRI. When CT is performed, axial spiral datasets are acquired before and after contrast administration; they are computed with a soft-tissue kernel, and multiplanar reconstructions should be performed. Usually, soft-tissue tumors larger than 5 mm can be detected by means of differences in absorption, the displacement they cause, and their obliteration of compartments. There are specific CT criteria on the hand for ganglion cysts and epidermal inclusion cysts, which have the same density as water; for lipomas with density values around −100 HU; for schwannomas and neurofibromas with intense contrast enhancement; and for heterodense fibrolipomas of the median nerve. An advantage in comparison to other procedures is the sensitive identification of calcifications within the tumor.
Magnetic Resonance Imaging
Because of its excellent soft-tissue contrast and the possibility of obtaining multiplanar images, MRI is the method of choice for the diagnosis of soft-tissue tumors of the hand:
Tumor identification: Soft-tissue tumors can be recognized by morphological criteria and alterations in signal intensity. The tumors usually lead to a lengthening in relaxation times, i.e., they appear hypointense in T1-weighted sequences and hyperintense in T2-weighted sequences. Exceptions will be explained.
Tumor expansion: Tumor delineation from the surrounding edema can best be achieved with T2-weighted FSE sequences (better than with T2*-weighted GRE sequences), as well as with fat-saturated T1-weighted SE sequences after intravenous administration of gadolinium. Infiltrations of the bone marrow can be sensitively identified in T1-weighted images and in the STIR sequence.
Tumor entity: Many soft-tissue tumors can be classified according to MRI criteria. MRI provides characteristic appearance for ganglion cysts (signal equivalent to fluid), lipomas (hyperintense in T1-weighted and T2-weighted sequences, fat-suppressed), peripheral neural tumors (hyperintense in T2 weighted sequences, heterodense enhancement), hemangiomas (vascular convolutes with contrast enhancement), and pigmented, villonodular synovitis (hypointense hemosiderin inclusions resulting from hemorrhage). Indistinct borders and inhomogeneous signal intensity within the tumor are in many cases indicative of malignancy, although a number of malignant tumors have unspecific findings.
Assessment Parameter | Evaluation |
Tumor size |
|
Tumor borders |
|
Regional spread |
|
Signal intensity in unenhanced MRI |
|
Signal homogeneity in unenhanced MRI |
|
Contrast enhancement |
|
Pattern of contrast enhancement |
|
Tumor necrosis |
|
For characterization of soft-tissue tumors in MRI diagnosis, the criteria in Table 45.1 should be analyzed and described.
Arteriography
Catheter angiography is only indicated for preoperative or preinterventional diagnosis of arteriovenous malformations and highly vascular tumors to determine the arterial feeder, as well as the draining veins. The other indications for arteriography of the hand are for circulatory disturbances (Chapter 48).
Disease Entities
Tumors of Cutaneous Origin
Epidermal Inclusion Cyst
Pathoanatomy and Clinical Symptoms
Synonyms are epithelial cysts and epitheloid cysts. The distended, elastic inclusions in the palm and on the palmar side of the fingers contain proteins, cholesterol, and lipoids; their walls are lined with squamous cells. The causation is assumed to be traumatic implantation of epidermis into the deeper layers of soft tissue. Male manual workers are most often affected.
Diagnostic Imaging
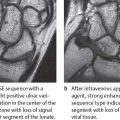
Due to their high fat and protein content, epidermal inclusion cysts do not necessarily appear cystic in sectional images. In US examinations the interior of the cysts can be anechoic to moderately echoic, with partially inhomogeneous echogenicity. Density values in CT are over 30 HU. The high protein content leads to a moderate decrease in signal intensity in comparison to pure cysts in T2-weighted sequences and to an intermediate signal intensity in T1-weighted sequences. Peripheral contrast enhancement can be seen ( Fig. 45.1 ). The subcutaneous location and capsular border, together with the patient’s history, indicate the correct diagnosis, though it is not possible to differentiate an epidermal inclusion cyst from an sebaceous cyst with MRI ( Fig. 45.2 ).


Cutaneous Carcinomas
Pathoanatomy and Clinical Symptoms
Almost 10% of cutaneous malignomas are found on the hands and feet. These include squamous-cell carcinomas, which have a preferred location on the nail fold, basal-cell epitheliomas, different forms of malignant melanoma with a predilection for subungual infiltration, and the rare Merkel-cell tumors.
Diagnostic Imaging
Sectional imaging (MRI, US) only indicated for better therapy planning of advanced cutaneous carcinomas. MRI offers significant advantages for local staging because of its better soft-tissue contrast ( Fig. 45.3 ). The depth of infiltration, especially the involvement of tendons, nerves, and blood vessels, can be determined with MRI. Staging of regional lymph nodes can be performed easily and reliably with high-resolution US.
Tumors Originating from Connective Tissue
Ganglion Cyst
Pathoanatomy and Clinical Symptoms
This most common soft-tissue tumor of the hand (up to 60%) is a accumulation of mucoid fluid within a capsule consisting of connective tissue. The pathogenesis has not been completely clarified; degeneration of periarticular connective tissue, synovial herniation, and repetitive injuries have been suggested. Ganglion cysts have no lining of synovial membrane. They are mostly found near joints and tendon sheaths. Approximately two-thirds of ganglion cysts are located on the back of the hand, with a predisposition for the immediate vicinity of the dorsal segment of the scapholunate ligament (Fig. 45.4c). The second most common localization is the space between the ligaments of the flexor carpi radialis and the abductor pollicis longus muscles. Ulnopalmar ganglion cysts are rare, as are those originating from tendons or anular ligaments. Women and adults between the ages of 20 and 40 years are predominantly affected. About half of the ganglion cysts cause no complaints; the rest cause pain, dysesthesias, or functional restriction. Pressure on the ligament of origin or the distal fibers of the posterior interosseous nerve can cause chronic pain. While large ganglion cysts are easy to diagnose with palpation, the small ones, which are mostly located in the dorsal capsule, are often not discovered in clinical examination.
Diagnostic Imaging
Radiographs can exclude intraosseous portions of ganglion cysts and are usually unremarkable. Refer to Chapters 23, 43, and 44 for more information on intraosseous ganglion cysts. Only large, paraosseous ganglion cysts cause periosteal and osseous reactions (scalloping) with superficial, smooth excavations, marginal osteosclerosis, and new bone formation. Clinically occult ganglion cysts at least 3 mm in size can be seen in US (Fig. 45.4a) and MRI (Fig. 45.4b, d, e). An advantage of MRI is that it can precisely demonstrate the surroundings of the ganglion cyst (joint capsule, tendon sheath, vessels, and nerves) and determine the site of origin. Table 45.2 summarizes the diagnostic criteria in MRI.

The use of US first in diagnosis of ganglion cysts is recommended because of the variable choice of imaging planes and low cost. Compression under visual control in US helps to differentiate between the only slightly deformable ganglion cyst and the displaceable joint effusion. Color Doppler US remains the procedure of choice to differentiate a ganglion cyst lying next to the radial artery from an aneurysm of the vessel (see Fig. 48.13 ). Occasionally, hypoechoic structures of the scapholunate joint space, the articular cartilage of the lunatum, and the dorsal radiotriquetral ligament can be confused with a ganglion cyst.
Small dorsal ganglion cysts, which can cause persistent complaints, and complicated ganglion cysts following trauma or infection can be reliably detected with T2-weighted MRI sequences. After administration of gadolinium there is peripheral contrast enhancement, although ganglion cysts are not lined with synovial tissue.

CT and arthrography can usually confirm transcortical communication between the extraosseous and intraosseous portions of the ganglion cysts.
Lipoma
Pathoanatomy and Clinical Symptoms
This fatty tumor has predisposed locations within the thenar and hypothenar muscles, as well as in the palm and on the proximal phalanges. Depending on the site of origin, endovaginal (originating from a tendon sheath) lipomas are differentiated from epivaginal ones. This soft tumor causes either no or only discrete symptoms from pressure on surrounding tissue.
Diagnostic Imaging
Large lipomas can be recognized in radiographs by a radiolucent zone – Bufalini sign (Fig. 45.5a). Calcifications are seldom found inside the tumor. Lipomatous tissue can be reliably identified in sectional imaging:
In US, the lipomatous space-occupying lesion is homogeneously hyperechoic and deformable.
In CT, absorption values between −80 and −120 HU and the lack of contrast enhancement confirm the presence of a lipoma.
In MRI, lipomas and subcutaneous fatty tissue are characteristically hyperintense in T1- and T2-weighted sequences. The signal intensity can be suppressed by fat-saturated sequences (Fig. 45.5b, c).
US
|
MRI
|
CT
|
If the homogeneous internal structure of a lipoma is not seen in any of these imaging modalities, a liposarcoma must be excluded.


Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


