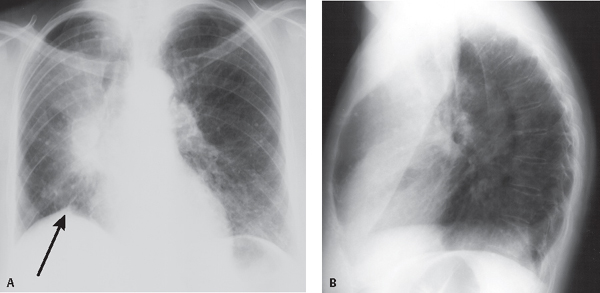
CASE 45 62-year-old woman with cough, weight loss, and generalized fatigue PA (Fig. 45.1A) and lateral (Fig. 45.1B) chest radiographs demonstrate opacification of the upper half of the right chest with cephalad displacement of the hilum and silhouetting of the ascending aorta and right heart border. A juxtaphrenic peak (arrow) is created by tethering of the inferior accessory fissure. The lateral exam also reveals marked anterior displacement of the oblique fissure. The displaced fissure is convex posteriorly. The right diaphragm is elevated and the mediastinum is shifted rightward. Combined Right Upper and Middle Lobe Atelectasis; Small Cell Lung Cancer • Mucus Plug • Primary Lung Cancer • Carcinoid Tumor • Metastatic Tumors • Neoplastic or Reactive Lymphadenopathy • Inflammatory Disease Fig. 45.1 Combined simultaneous collapse of the right upper and middle lobes is uncommon because of the disparate location of their lobar bronchi. Thus, two different diseases or a single disease simultaneously involving these two separate bronchi must be considered. Bilobar collapse is most often described in the setting of mucus plugs with concomitant primary lung cancer, primary lung cancer with associated reactive or neoplastic lymphadenopathy, metastatic disease, carcinoid tumors, or inflammatory strictures.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


