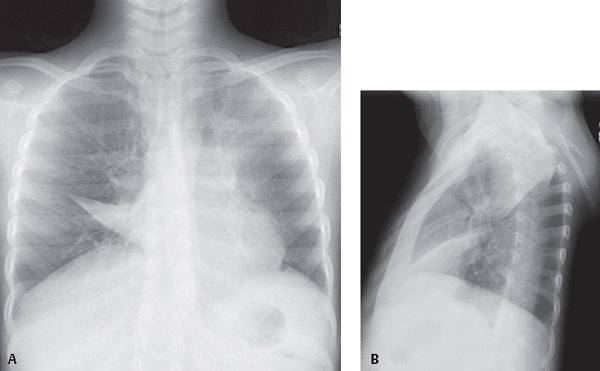
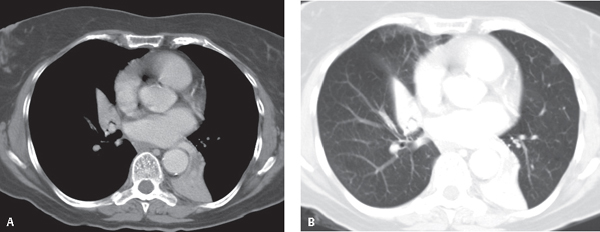
CASE 46 Asthmatic child with an acute exacerbation PA (Fig. 46.1A) and lateral (Fig. 46.1B) chest radiographs reveal abnormal opacities in each hemithorax. The frontal exam (Fig. 46.1) demonstrates an ill-defined left parahilar opacity silhouetting the upper left heart border. Note the absence of air bronchograms, ipsilateral mediastinal shift, and juxtaphrenic peak. This exam also shows a triangular opacity silhouetting the right heart border. The apex of this opacity is directed away from the hilum. The upper thorax on the lateral exam (Fig. 46.2) demonstrates a triangular opacity with its apex at the hilum and its base contiguous with the parietal pleura posterior to the extreme apex of the hemithorax (mediastinal wedge). Note the anterior displacement of the left oblique fissure. More inferiorly, a thin triangular opacity extends from the retrosternum toward the hilum. The horizontal fissure is displaced inferiorly and the right oblique fissure anteriorly Combined Right Middle Lobe and Left Upper Lobe Atelectasis; Mucus Plugs Fig. 46.1 (Images courtesy of Lakshmana Das Narla, MD, VCU Medical Center; Richmond, Virginia.) Fig. 46.2 Contrast-enhanced chest CT (A, mediastinal window; B, lung window) of a 68-year-old woman with asthma, chronic cough, and allergic bronchopulmonary aspergillosis (ABPA) reveals total collapse of the right middle and left lower lobes. Note the mucus-filled bronchi in the collapsed left lower lobe. Affected patients may suffer from asthma and often present with bronchospasm, initially episodic but later becoming more chronic (Images courtesy of Malcolm K. Sydnor, MD, VCU Medical Center; Richmond, Virginia). • Non-Neoplastic Causes of Multi-Lobar Collapse • Neoplastic Disease The double lesion
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Mucus Plugs
Mucus Plugs
 Aspirated Foreign Bodies
Aspirated Foreign Bodies
 Post-Infectious or Post-Inflammatory Strictures
Post-Infectious or Post-Inflammatory Strictures
 Discussion
Discussion
Background
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine



