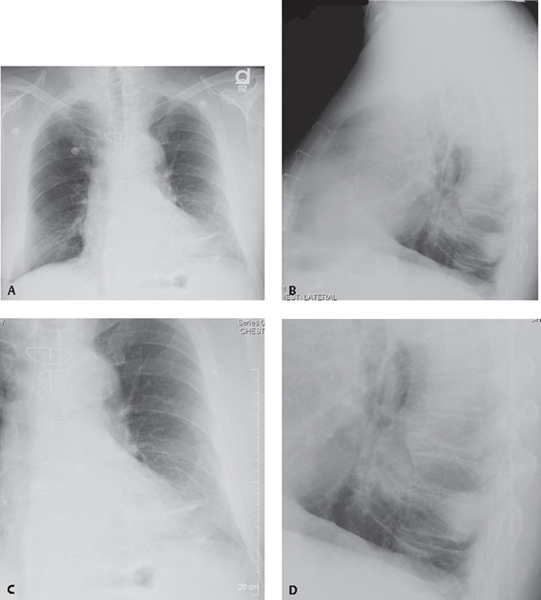
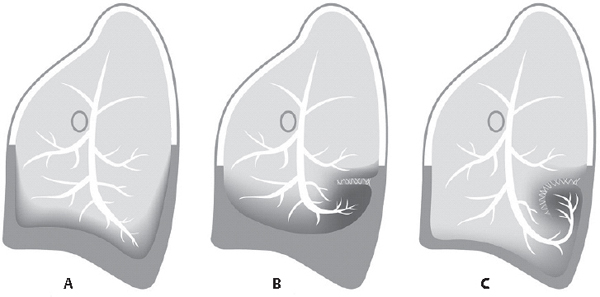
CASE 48 77-year-old man formerly employed as a construction site foreman with long-standing history of tobacco abuse complains of chronic cough PA (Fig. 48.1A) and lateral (Fig. 48.1B) chest radiographs show a 3.0 cm mass in the retrocardiac region of the left lower lobe. On the coned-down frontal exam (Fig. 48.1C), the margins of the mass are poorly defined, suggesting it is pleural based. The coned-down lateral exam (Fig. 48.1D) shows adjacent vessels and bronchi curving into the medial edge of this mass. Note the adjacent pleural thickening. Fig. 48.1 Rounded Atelectasis Synonyms • Round Atelectasis • Folded Lung • Asbestos Pseudotumor • Primary Lung Cancer • Secondary Lung Cancer • Pneumonia Rounded atelectasis is a distinct form of relaxation atelectasis seen in association with focal pleural thickening. Decortication of the adjacent pleura is often associated with re-expansion of this focally atelectatic lung. Two hypotheses have been proposed for the development of rounded atelectasis. The first is predicated on a pre-existent pleural effusion (Fig. 48.2A). The effusion causes the adjacent lower lobe to float upward and compresses the lung. A cleft or fold then occurs in the visceral pleura (Fig. 48.2B). The lung then begins to tilt and curl on itself in a concentric fashion along this cleft (Fig. 48.2C). Fibrinous adhesions along this cleft suspend the atelectatic segment (Fig. 48.2C). As the effusion resorbs, aerated lung fills in the space around the focal “rounded” atelectatic lung. Organization of the fibrinous exudate and fibrous contraction cause the affected lung to remain “balled up” as a mass-like lesion (Fig. 48.2C). The second hypothesis suggests an irritant (e.g., asbestos) induces a local pleuritis, causing the pleura to thicken and contract. The adjacent lung “shrinks,” and the atelectasis develops in a rounded mass-like configuration. Most cases of rounded atelectasis occur in patients with a history of asbestos exposure. Other manifestations of asbestos exposure may be observed in such patients (e.g., pleural plaques) (Figs. 48.3A, 48.3B). However, rounded atelectasis has also been described in association with pleural effusions of tuberculous and non-tuberculous etiologies, pulmonary infarction, iatrogenic pneumothorax, heart failure, coronary artery revascularization, talc pleurodesis, malignant pleural disease, etc. Most patients are asymptomatic and the lesion is often an incidental radiologic finding. Rounded atelectasis most frequently occurs in the lower lobes (55% of cases). Less frequent presentations occur in the middle lobe and lingula (39% of cases) and in the upper lobes (6% of cases). Fig. 48.2
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Clinical Findings
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine



