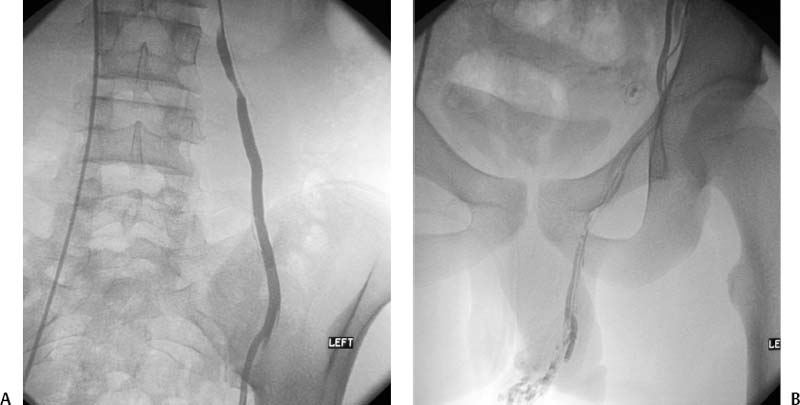
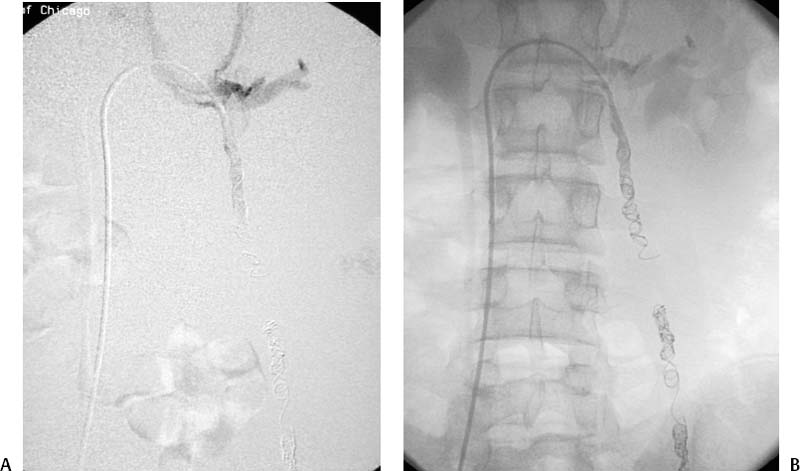
CASE 49 A 25-year-old male presented with left-sided scrotal pain and swelling. He underwent scrotal ultrasound. Figure 49-1 Scrotal sonography in a 25-year-old male with left-sided swelling shows a varicocele. Figure 49-2 Conventional venography. (A) Injection of the left spermatic vein just below the renal vein confluence shows reflux of contrast material to the sacroiliac level. (B) A more caudal image shows reflux of contrast into dilated veins within the scrotum. Initial sonographic interrogation of the scrotum revealed multiple serpiginous veins showing marked increase in color flow during the Valsalva maneuver (Fig. 49-1). Selective venography of the left spermatic vein from the femoral vein approach revealed retrograde reflux of contrast to the level of the scrotum. Multiple distended veins within the scrotum were opacified (Fig. 49-2). Figure 49-3 Selective spermatic venography after successful embolization using coils. (A) Digital subtraction image shows antegrade flow of contrast into the renal vein without caudal reflux into the spermatic vein or collateral veins. (B) Unsubtracted image shows coil embolization of the entire length of the left spermatic vein to prevent recurrence by collateral vein recruitment. Left-sided varicocele resulting from valvular incompetence within the spermatic vein. The right common femoral vein was accessed using the Seldinger technique, and a 5-French (F) vascular sheath was inserted. Using a 5F Cobra catheter (Cook, Bloomington, Indiana) and standard guidewire, the left renal vein and subsequently the left spermatic vein were catheterized. Contrast material was injected into the spermatic vein near the level of the renal vein, reflux of contrast to the level of the scrotum was observed, and the varicocele was opacified. The catheter was advanced to a point below the sacroiliac level, and coils were deployed throughout the spermatic vein. Follow-up venography revealed no opacification of the spermatic vein (Fig. 49-3). The patient was discharged after a 5-hour observation period, and he reported marked reduction in scrotal distention within 1 week. An 8-month follow-up evaluation revealed no evidence of recurrence of the pain or the varicocele. Varicoceles are networks of dilated veins of the pampiniform plexus within the scrotum, often described on physical exam as a “bag of worms.” This abnormality occurs in approximately 15% of males at or above puberty, is left-sided in 90% of cases, and is bilateral in approximately 8%. The pathogenesis involves either reflux into the spermatic vein caused by valvular incompetence (most common), outflow obstruction of the left renal vein and spermatic vein caused by compression of the renal vein between the aorta and superior mesenteric artery (Nutcracker phenomenon), or abnormal supply to the pampiniform plexus by anomalous veins. Anomalous veins include valveless collaterals between the spermatic vein and segmental renal veins or retroperitoneal veins. In addition, the spermatic vein itself can be composed of multiple branches, sometimes communicating separately with the renal vein, lumbar veins, or retroperitoneal veins.
Clinical Presentation

Radiologic Studies
Diagnosis
Treatment
Equipment
Discussion
Background
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


