
Phospholipase-Associated Neurodegeneration (PLAN)
Primary Diagnosis
Phospholipase-associated neurodegeneration (PLAN)
Differential Diagnoses
Lysosomal storage disorders
Mitochondrial disorders
Defects of carbohydrate glycosylation
Imaging Findings
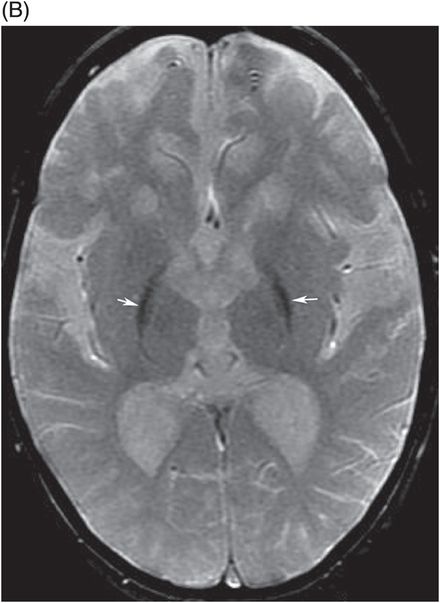
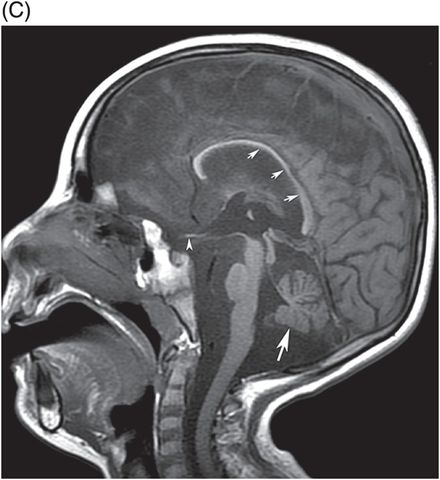
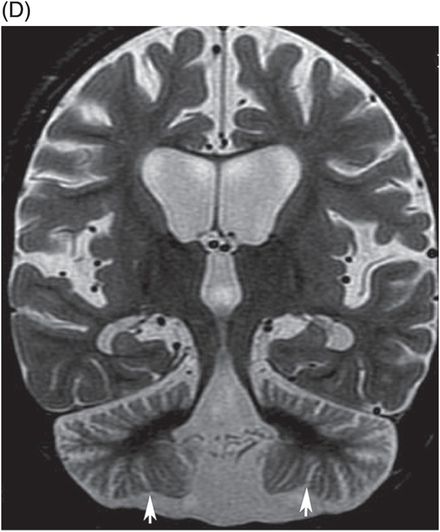
Fig. 5.1: (A) Axial T2WI through the level of basal ganglia demonstrated T2 hypointensity (arrows) secondary to iron deposition involving bilateral putamen, globus pallidi, and severe cerebral atrophy for an 18-month-old as evidenced by the enlargement of the ventricles and cerebral sulci. (B) Axial GRE image through the same level demonstrated more pronounced hypointensity involving bilateral basal ganglia (arrows), confirming iron deposition. (C) Midline sagittal T1WI demonstrated severe atrophy of the vermis (large arrow), thinning of the corpus callosum (small arrows), and optic chiasm (arrowhead). (D) Coronal T2WI through the cerebellum also demonstrated severe atrophy of bilateral cerebellar hemispheres (arrows). (E) Coronal MR image through the level of the sella demonstrates atrophy of the optic chiasm (arrowheads).
Discussion
This patient has the typical clinical and radiologic presentation of phospholipase-associated neurodegeneration (PLAN). Relatively rapid-onset motor signs, severe muscular weakness, regression of language and motor skills, and visual disturbances that developed after birth are typical clinical presentations of PLAN. A diagnosis of PLAN is more certain with the characteristic radiologic findings seen in this case including diffuse cerebellar atrophy, optic atrophy, thin corpus callosum, and evidence of iron deposition in the basal ganglia.
Cerebellar atrophy and retinal degeneration can be a manifestation of a wide variety of congenital errors of metabolism including lysosomal storage disorders, mitochondrial disorders, and defective carbohydrate glycosylation. Although optic atrophy can be part of these inborn metabolic errors, abnormal iron deposition is not a feature of these disorders. In patients without abnormal iron deposition, the diagnosis can be difficult: metabolic and genetic screening should be performed to establish a definitive, correct diagnosis.
PLAN is due to mutation of the calcium-independent phospholipase A2 gene (PLA2G6). Phenotypic presentation of PLAN can be infantile, before two years of age, and has been variably referred to in the literature as infantile neuroaxonal dystrophy (INAD), Seitelberger disease, and neurodegeneration with brain iron accumulation (NBIA) 2A in Online Mendelian Inheritance in Man® (OMIM®, http://www.omim.org) (OMIM #256600). PLAN can have atypical presentation, referred to as atypical PLAN, with delayed presentation, usually manifesting after three years of age. This atypical PLAN has also been described in literature as atypical neuroaxonal dystrophy (ANAD).
Both typical and atypical PLAN patients are asymptomatic at birth. Over time, they develop developmental delay. In typical PLAN, patients develop language and motor regression, diffuse muscular weakness and hypotonia, followed by spastic quadriplegia. Muscular weakness can be so severe that feeding and breathing may be difficult and patients frequently develop pneumonia. Optic atrophy results in visual disturbances and nystagmus is commonly present. Like other NBIA subtypes, the atypical form is slowly progressive as compared to the typical presentation. Atypical PLAN is characterized by movement disorders and dystonia with or without pyramidal symptoms.
The dominant imaging finding, present in all typical PLAN cases, is cerebellar atrophy that involves both the vermis as well as the cerebellar hemispheres and usually precedes the inconsistent abnormal iron deposition that can be seen in up to 50% of patients. Iron deposition typically occurs in the globus pallidus. Optic atrophy is another typical imaging manifestation and can best be evaluated in coronal T2 STIR sequences. The corpus callosum appears thin, particularly the splenium, which appears smooth and may be vertically oriented (slit-like). Unlike other NBIA subtypes, diffuse FLAIR hyperintensity in the deep white matter is not a feature of PLAN.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


