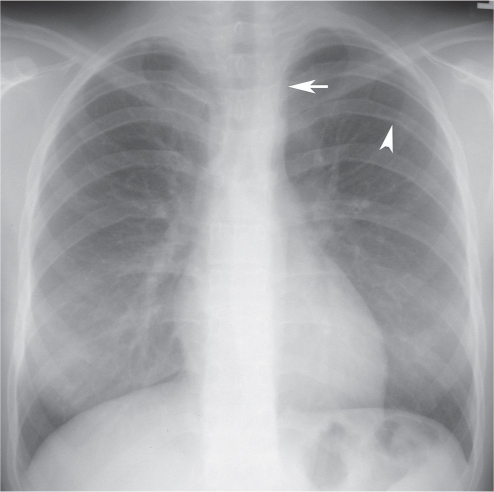
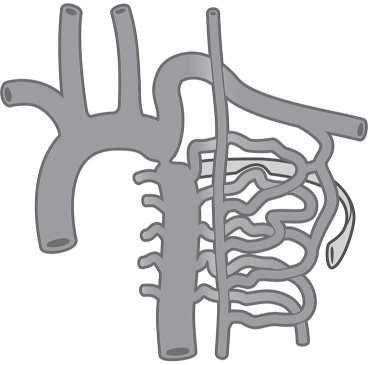
CASE 5 18-year-old woman with differential upper and lower extremity blood pressures and stronger radial than femoral pulses PA (Fig. 5.1) chest radiograph demonstrates rib notching (arrowhead) and an inconspicuous aortic arch. The heart size and pulmonary vascularity are normal. The straight left superior mediastinal contour (arrow) is formed by an enlarged left subclavian artery. Artist’s illustration (Fig. 5.2) depicts the collateral pathways that produce dilatation and tortuosity of the intercostal arteries and the radiographic finding of rib notching, which results from benign pressure erosion by the pulsatile collateral vessels on the adjacent ribs. Coarctation of the Aorta • Pseudocoarctation • Neurofibromatosis • Pulmonary Atresia with Harvested Systemic Vessels Communicating with Pulmonary Vessels Fig. 5.1 Fig. 5.2 Coarctation of the aorta is a focal luminal narrowing distal to the left subclavian artery near the ligamentum arteriosum. Such luminal narrowing can be focal (coarctation), diffuse (hypoplastic isthmus), or complete (aortic interruption). It accounts for approximately 6% of congenital cardiac anomalies. While there is blood flow across the coarctation, it is supplemented by collateral blood flow that bypasses the obstruction through the spinal artery, intercostal arteries (Fig. 5.2), epigastric arteries, lateral thoracic artery, and periscapular arteries. These collateral vessels are not usually present at birth and develop over time. Coarctation of the aorta is a congenital anomaly of unknown etiology. Diffuse coarctation is thought to result from marked reduction of blood flow through the fetal aortic isthmus from associated congenital cardiac anomalies.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


