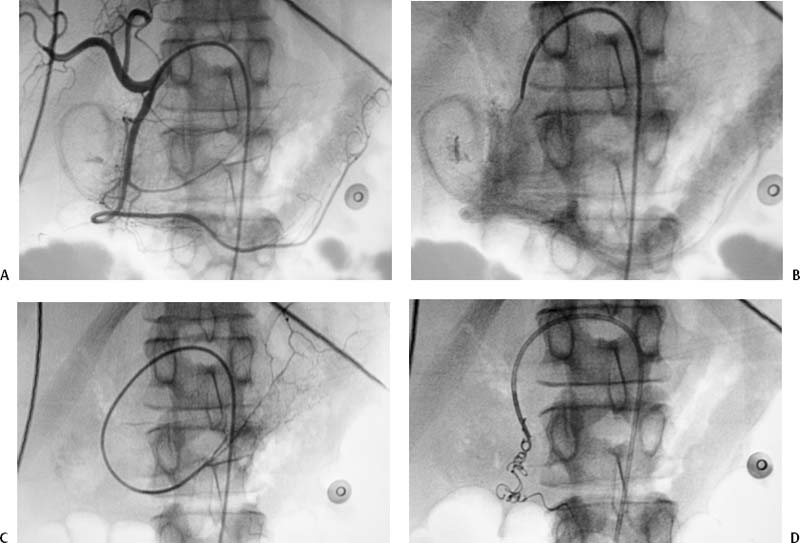
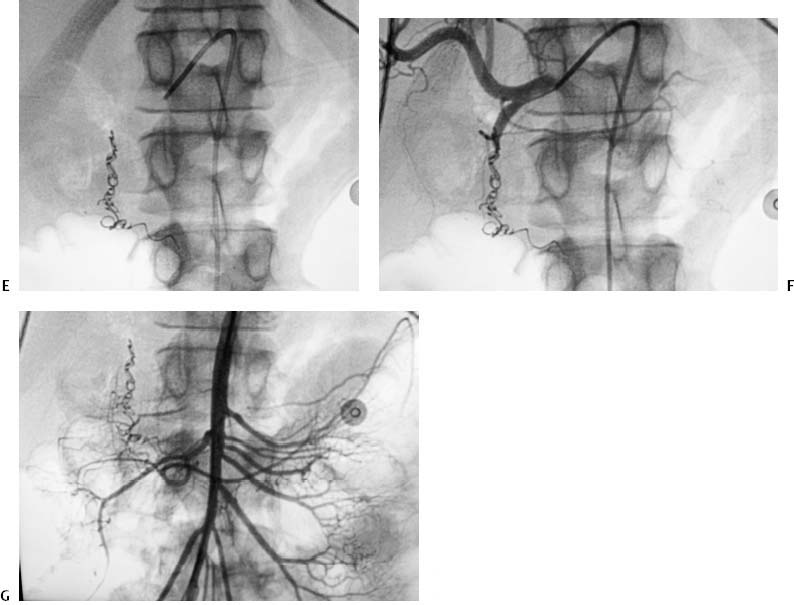
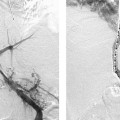
CASE 5 A 54-year-old female with massive hematemesis was admitted to the intensive care unit and underwent emergent upper endoscopy. This revealed a bleeding duodenal ulcer. Hemorrhage could not be controlled using endoscopic therapy. The patient was then referred to interventional radiology. Figure 5-1 Embolization of the gastroduodenal artery in a patient with duodenal hemorrhage. (A) Common hepatic arteriogram shows focus of extravasation in the region of the duodenum. (B) Venous phase of common hepatic arteriogram shows persistent pooling of blood from gastroduodenal artery indicating hemorrhage. (C) Gastroepiploic arteriogram shows catheter advanced beyond the focus of bleeding. (D) Fluoroscopic image early shows coil embolization of gastroduodenal artery. (E) Fluoroscopic image shows complete coil embolization of gastroduodenal artery. (F) Common hepatic arteriogram after embolization shows occlusion of the gastroduodenal artery. (G) Superior mesenteric arteriogram shows no evidence of backbleeding to embolized gastroduodenal artery. The right common femoral artery was punctured using the Seldinger technique and a 5-French (F) sheath was inserted. Through the sheath, an RC-1 (Boston Scientific, Natick, Massachusetts) catheter was used to selectively catheterize the common hepatic artery and an angiogram was performed, revealing contrast extravasation from the gastroduodenal artery (Figs. 5-1A, B). Bleeding duodenal ulcer. The catheter was advanced into the gastroepiploic artery beyond the site of bleeding in the gastroduodenal artery (Fig. 5-1C). Coils and Gelfoam (Pharmacia and Upjohn, Kalamazoo, Michigan) pledgets were deployed across the bleeding site in the gastroduodenal artery (Figs. 5-1D, E). A postembolization common hepatic arteriogram revealed cessation of bleeding (Fig. 5-1F). The catheter was then used to select the superior mesenteric artery, and angiography was performed revealing no hemorrhage from retrograde flow (Fig. 5-1G). 5F vascular sheath 5F mesenteric catheters (RC-1, RIM, VS-1) 0.035” conventional and hydrophilic soft-tipped guidewires Contrast material Embolization coils (3- to 6-mm diameter) Gelfoam (Pharmacia and Upjohn, Kalamazoo, Michigan) Microcatheters and microcoils (rarely necessary)
Clinical Presentation
Radiologic Studies
Angiography
Diagnosis
Treatment
Equipment
DISCUSSION
Background
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


