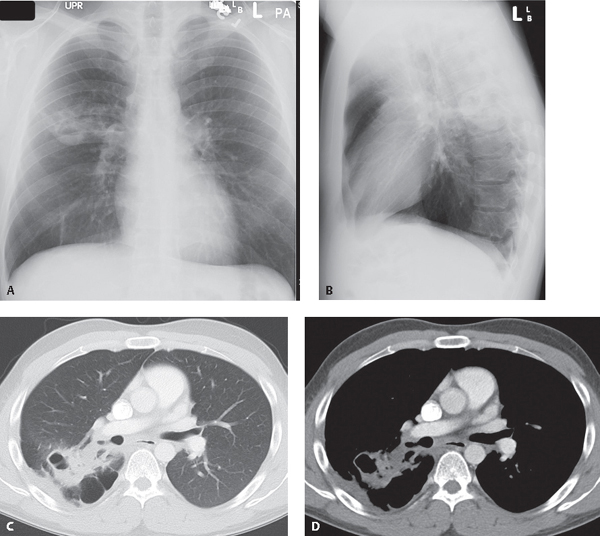
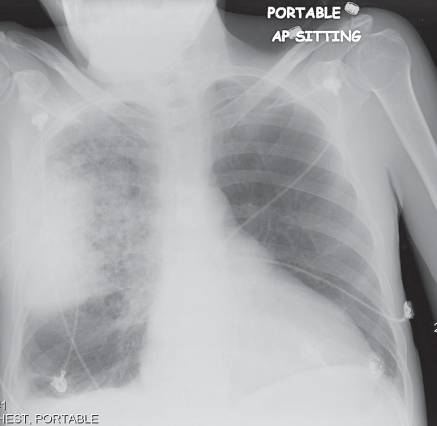
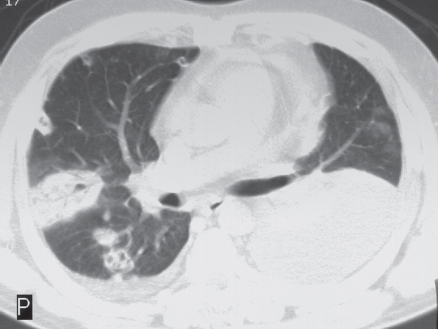
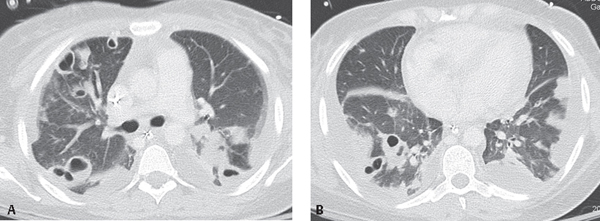
CASE 50 26-year-old man with fever, cough productive of purulent sputum, and hemoptysis PA (Fig. 50.1A) and lateral (Fig. 50.1B) chest radiographs demonstrate a patchy area of consolidation with associated cavitation and surrounding ground glass in the superior segment right lower lobe. Contrast-enhanced chest CT (Fig. 50.1C, lung window; Fig. 50.1D, mediastinal window) shows a corresponding focus of ill-defined parenchymal consolidation with surrounding ground glass and adjacent pleural thickening. Note the low-attenuation areas (Fig. 50.1D), reflecting regions of necrosis and the cavitation. Paraseptal emphysema parallels the costovertebral pleura (Fig. 50.1C). Fig. 50.1 Staphylococcal Pneumonia; Superior Segment Right Lower Lobe • Other Community-Acquired Bronchopneumonias Pulmonary infection occurs through hematogenous spread or aspiration of contaminated oral secretions. Twenty to 40% of older children and adults, and more than 50% of health care workers, are nasal carriers of staphylococci. S. aureus causes less than 5% of community-acquired pneumonias, but is responsible for more than 10% of hospital-acquired pneumonias. Staphylococcal pneumonia often complicates viral pneumonias (e.g., influenza) in adults (Fig. 50.2) and measles in children. Aspiration can lead to pneumonia in intubated patients and in those with underlying COPD or lung cancer. Patients with contaminated vascular catheters and those with endocarditis (Fig. 50.3) or intravenous drug abuse (IVDA) history (Figs. 50.4A, 50.4B) may have hematogenous spread to the lungs. Staphylococcal pneumonia is caused by the Gram-positive bacteria Staphylococcus sp. S. aureus is responsible for most cases of staphylococcal bronchopneumonia. Staphylococci produce toxins causing significant tissue destruction and lung abscesses (Figs. 50.1A, 50.3, 50.4. 50.5, 50.6). The inflammatory exudate is multifocal and fills the large airways, following the course of the tracheobronchial tree. Consolidation is usually segmental and is characterized by segmental volume loss and the absence of air bronchograms. Fig. 50.2 AP chest radiograph of a 57-year-old man with methicillin-resistant Staphylococcus aureus (MRSA) pneumonia complicating recent influenza reveals an ill-defined right perihilar bronchopneumonia with peripheral air space consolidation. A small ipsilateral pleural effusion is present. Fig. 50.3 Chest CT (lung window) of a 41-year-old patient with tricuspid valve murmur, fever, and S. aureus endocarditis shows multiple intraparenchymal and juxtapleural nodules, and consolidations of variable size consistent with septic emboli. Many lesions are cavitated, and some exhibit associated feeding vessels supporting a hematogenous route of dissemination. Fig. 50.4 Chest CT (lung window) through the (A) upper and (B)
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


50 Staphylococcus Pneumonia




