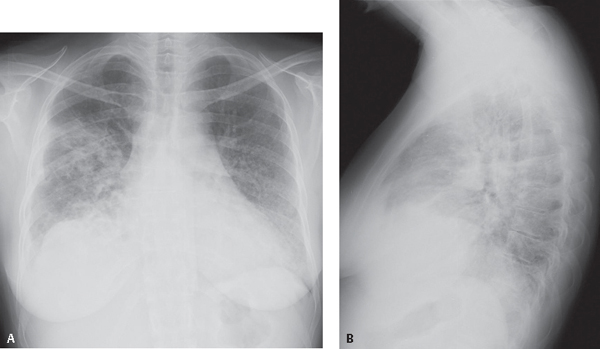
CASE 51 42-year-old woman with long-standing history of poorly controlled diabetes presented to the Emergency Department with purulent productive cough, shortness of breath, and fever PA (Fig. 51.1A) and lateral (Fig. 51.1B) chest X-rays demonstrate poorly defined nodular opacities and patchy areas of consolidation and a small right pleural effusion. Sputum and blood cultures confirmed the diagnosis. Haemophilus influenzae Pneumonia • Other Community-Acquired Bronchopneumonias Fig. 51.1 H. influenzae pulmonary infection is acquired through person-to-person transmission via aerosolized droplets deposited in the nasopharynx. The nasopharynx is colonized in up to 90% of children by 5 years of age. Many patients with COPD are also colonized. The pleomorphic, Gram-negative bacterium Haemophilus influenzae causes Haemophilus pneumonia. Most organisms that colonize the nasopharynx are unencapsulated and non-typeable. Most strains that infect the lung are encapsulated and typeable. Type b is the most common strain responsible for Haemophilus pneumonia (Hib). H. influenzae
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


