Axial T2WI at the level of the lateral ventricles.
Axial DWI.
Balo Concentric Sclerosis
Primary Diagnosis
Balo concentric sclerosis
Differential Diagnoses
Glioma
Metastasis
Multiple sclerosis
Encephalitis
Infections (fungal and pyogenic)
Imaging Findings
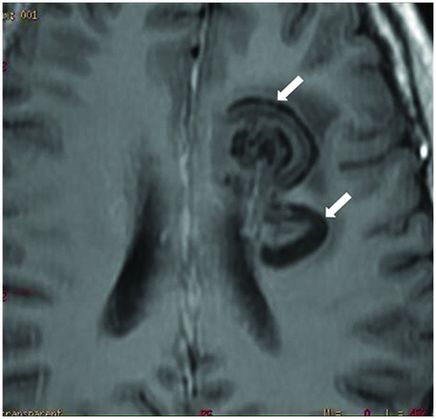
Fig. 57.1: Axial T2WI at the level of the lateral ventricles demonstrated two oval-rounded lesions in the deep and periventricular white matter of the left frontal lobe. Mild adjacent edema (white arrows) noted but no significant effect. Note that the larger lesion (bold arrow) showed the typical lamellar pattern with alternating hypo- and hyperintense bands. Fig. 57.2: Axial enhanced T1WI showed that the larger lesion (arrow) is associated with blood-brain barrier breakdown, which also demonstrated incomplete ring of enhancement in a horseshoe configuration. Fig. 57.3: Axial DWI showed high intensity signal with a round configuration at the same level as the enhancement, and inside the lesions proper. The ADC values were mildly lower than in the contralateral white matter (image not shown). Fig. 57.4: Axial enhanced T1-weighted image posterior to seven-day treatment with steroids (1.5-month follow-up). Both lesions (arrows) no longer showed contrast enhancement, but still show the lamellar pattern with onionskin appearance.
Discussion
A clinicoradiologic picture of acutely progressive neurologic deficits is not expected in patients with a primary or secondary brain tumor, which more commonly demonstrate a more subacute presentation. Patients with multiple sclerosis (MS) may show acute neurologic symptoms, which can be seen during the first attack of the relapsing-remitting form of MS. Primary progressive MS demonstrates steadily worsening neurologic symptoms, without episodic remission.
Acute, progressive neurologic deficits also present in patients with intracranial infections, such as encephalitis. However, patients with encephalitis typically show a more severe symptomatology, such as confusion, loss of consciousness, seizures, hallucinations, or even agitation. Certain fungal and pyogenic infections can cause acute progressing neurologic symptoms, which are usually associated with headache, fever, and a focal neurologic deficit. Patients with abscess can also present with nausea, vomiting, and neck stiffness if the meninges are also affected. In patients with intracranial infection, hematology studies typically demonstrate elevated WBC and SED levels; C-reactive protein level may be altered. Immunodeficient pathologies (such as AIDS) can be risk factors for opportunistic brain infections, such as toxoplasmosis and cryptococcosis.
Primary and secondary brain tumors typically demonstrate enhancement, active demyelination, and, possibly, infection on imaging studies. A horseshoe pattern (or open ring) of enhancement, combined with the presence of oligoclonal bands in CSF corroborate existence of a demyelinating process in this patient. The lamellar pattern (onionskin configuration) seen on both T2- and T1-weighted images (Figs. 57.1, 57.2, and 57.4) is typically seen in cases of Balo concentric sclerosis (BCS), which can be considered a pathognomonic finding in patients with this disease.
Balo concentric sclerosis, first described as encephalitis periaxialis concentrica by Jozsef Baló (a Hungarian neuropathologist) in 1927, is a rare form of MS. Initially, BCS was deemed comparable to the Marburg variant of MS, a monophasic disease with fast progression and a typically fatal patient outcome. Currently, BCS is no longer considered an unfailingly fatal condition, as an increasing number of authors have been reporting cases with prolonged survival and, occasionally, spontaneous resolution. Current literature reviews indicate that BCS is more comparable to the more classical form of MS (Charcot type) than Marburg variant MS disease.
Clinical symptoms of BCS include acute/subacute onset of mild cognitive impairment, altered behavior of focal neurologic deficits, which can endure for weeks or months – simulating a space-occupying lesion. Patients are typically young, and commonly present with headache, aphasia, cognitive or behavioral dysfunction, and/or seizures. Mononuclear inflammatory reaction and oligoclonal bands may be demonstrated in CSF studies.
On brain MRI, the imaging modality of choice, BCS findings consist of alternating hypo- and hyperintense concentric rings on T2-weighted images and contrast-enhanced T1-weighted images with a typical onionskin appearance (Figs. 57.1, 57.2, and 57.4). Postcontrast T1-weighted images superbly demonstrate the distinct rings of enhancement in a concentric pattern at the sites of blood-brain barrier breakdown.
In patients with early-stage BCS, MRI studies can be used to diagnose the disease accurately – significantly affecting patient morbidity and mortality associated with the disease. Currently, there is trend among radiologists to consider the distinctive MR findings of BCS as pathognomonic. If this trend continues, it will enable clinicians to provide an earlier diagnosis and recommended course of treatment, which may decelerate the inflammatory process and perhaps improve clinical outcome.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


