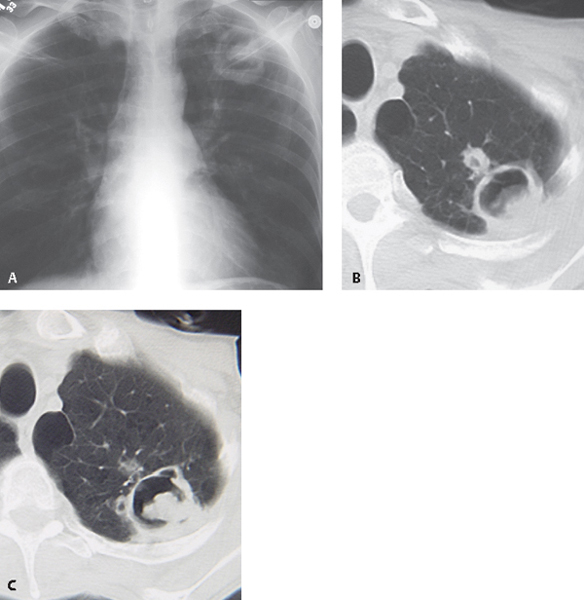
CASE 64 67-year-old man with hemoptysis and prior tuberculosis Coned-down PA chest radiograph (Fig. 64.1A) demonstrates a cavitary left apical lesion with an intrinsic soft-tissue nodule and an air-fluid level. Coned-down unenhanced chest CT (lung window) (Figs. 64.1B, 64.1C) demonstrates a left apical thick-walled cavitary lesion with an intrinsic dependent soft-tissue nodule and small cavitary satellite nodules. Note adjacent pleural thickening as well as left apical centrilobular and paraseptal emphysema. Aspergillosis; Mycetoma Fig. 64.1 • Mycetoma; Secondary to Other Fungi • Chronic Necrotizing Aspergillosis • Cavitary Lung Cancer with Necrotic Lung or Mycetoma Formation The fungi classified as Aspergillus species occur worldwide and may produce disease through colonization of abnormal lung tissue or through vascular and tissue invasion in immunocompromised individuals. Aspergillosis is typically caused by three major species of fungi: Aspergillus fumigatus, A. flavus, and A. niger. The clinical spectrum of Aspergillus infection is dependent upon the integrity of the host’s immune system (Table 64.1). Patients with saprophytic aspergilloma (mycetoma, fungus ball) usually have a normal immunity and abnormal lung parenchyma, typically cavitary lung disease often secondary to tuberculosis or sarcoidosis. These patients may be entirely asymptomatic or may present with hemoptysis, which may be massive. Angioinvasive aspergillosis typically occurs in patients with severe neutropenia (absolute neutrophil count <500 × 103/mL) who present with fever, dyspnea, cough, and chest pain. Chronic necrotizing (semi-invasive) aspergillosis affects patients with severe underlying lung disease who present with fever, productive cough, and dyspnea. Allergic bronchopulmonary aspergillosis is a hypersensitivity reaction (types I and III) to Aspergillus organisms in the tracheobronchial tree. Affected patients may have cystic fibrosis or chronic asthma and may present with wheezing, fever, productive cough, and chest pain. Aspergillus may produce necrotizing pseudomembranous tracheobronchitis (airway-invasive aspergillosis) in a small percentage of immunocompromised patients (neutropenia, AIDS) who present with dyspnea, wheezing, and cough. • Gravity-dependent soft-tissue nodule or mass within preexisting cavity • Air crescent sign: crescent of air along non-dependent aspect of cavity surrounding the mycetoma
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Imaging Findings
Radiography
Mycetoma (Fig. 64.1A)
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


