CASE 65 A 5-week-old boy presents to the emergency department with a 4-day history of nonbilious projectile vomiting. Figure 65A Longitudinal and transverse images of the pylorus (Figs. 65A1 and 65A2) demonstrate an elongated, thickened pylorus, with a muscle wall thickness of 5 mm. Fluid was seen within the gastric antrum, with no transit of gastric contents into the duodenum. Hypertrophic pyloric stenosis (HPS) HPS is an acquired hypertrophy of the circular muscle of the pylorus, causing progressive gastric outlet obstruction, It occurs with an incidence of ~3 per 1000 live births. There is an increased incidence in boys (male:female 4:1), first-born children, and Caucasian race. Some cases show a strong familial tendency. The etiology remains largely unknown, although abnormal innervation to the circular muscle has been implicated. Classically, infants present between 2 and 6 weeks of life with projectile nonbilious vomiting occurring 10 to 20 minutes after feeding. Occasional cases as early as the first week of life and as late as 5 months have been described. Infants fail to thrive and may become dehydrated. The classic metabolic abnormality of hypokalemic hypochloremic alkalosis is now rare. On clinical examination, gastric peristaltic activity may be seen and a palpable small mass, the “olive,” may be felt in the right upper quadrant, although earlier diagnosis has reduced the incidence of this finding over the past 2 decades.
Clinical Presentation
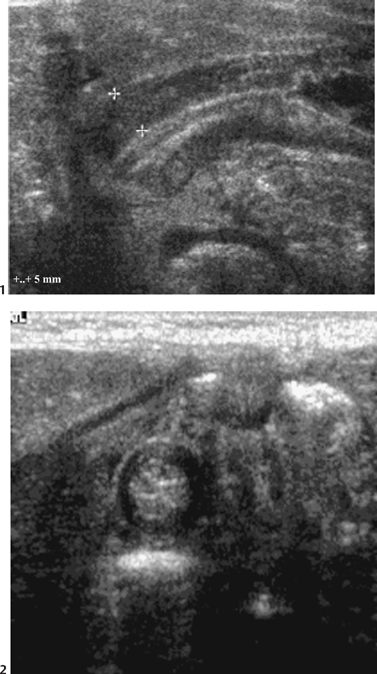
Radiologic Findings
Diagnosis
Differential Diagnosis
Discussion
Background
Etiology
Clinical Findings
Pathology
Imaging Findings
ULTRASOUND
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


