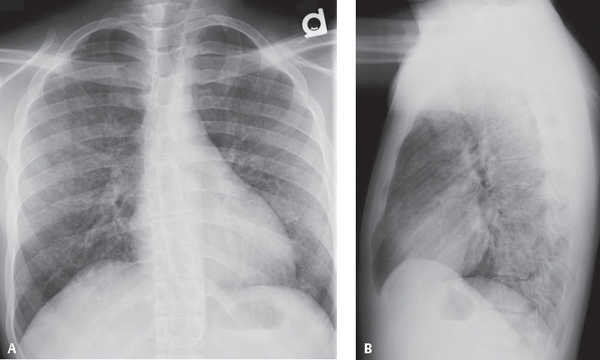
CASE 66 26-year-old man with HIV-AIDS, CD4 count of 14 cells/μL, fever, non-productive cough, and dyspnea PA (Fig. 66.1A) and lateral (Fig. 66.1B) chest radiographs demonstrate patchy, bilateral, perihilar ground glass and reticular-nodular opacities without lymphadenopathy or pleural effusions. Pneumocystis jiroveci Pneumonia • Mycoplasma Pneumonia • Various Viral Pneumonias • Mycobacterium avium Complex Pneumonia • Histoplasmosis Pulmonary Infection • Cryptococcus Pulmonary Infection • Lymphocytic Interstitial Pneumonia (LIP) Fig. 66.1 Pneumocystis pneumonia (PCP) is caused by the yeast-like fungus Pneumocystis jiroveci (yee-row-vet-zee), named after the Czech parasitologist Otto Jirovec. The organism was previously misclassified as a protozoan and called Pneumocystis carinii. However, use of that nomenclature is now considered incorrect, as Pneumocystis carinii infection only occurs in animals, not humans. Pneumocystis infection has a worldwide distribution. Pneumocystis is commonly found in the lungs of immunocompetent individuals but usually causes infections only in those with altered immune systems. Risk factors for pulmonary infection include congenital or acquired disorders of cell-mediated immunity, organ transplantation, chemotherapy for hematologic or lymphoreticular neoplasia, and AIDS. Pneumocystis jiroveci is the second most common cause of pneumonia in AIDS patients and infects up to 80% of patients at some time during the course of their illness. Pneumocystis pneumonia is an AIDS-defining diagnosis. Pneumocystis pneumonia is likely acquired through inhalation of airborne respiratory secretions. Pneumocystis jiroveci causes subclinical infection in most persons during childhood. Latent infection develops into opportunistic pneumonia when an individual becomes immunosuppressed. The possibility of person-to-person transmission has been suggested but not yet definitively proven. The clinical presentation of infected patients is variable. Signs and symptoms may be mild, but disease may be fulminant and may rapidly progress to respiratory failure. Patients with AIDS and Pneumocystis pneumonia tend to have a more indolent course. Non-productive cough (95%), dyspnea (95%), and fever (80%) are common symptoms and signs. Hypoxemia occurs in 80–95% of infected patients, and the DLCO is invariably diminished. Ninety percent (90%) of HIV-infected patients have an elevated lactate dehydrogenase (LDH) level, with a mean value of 375 ± 23 IU/L. Complications of Pneumocystis
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


