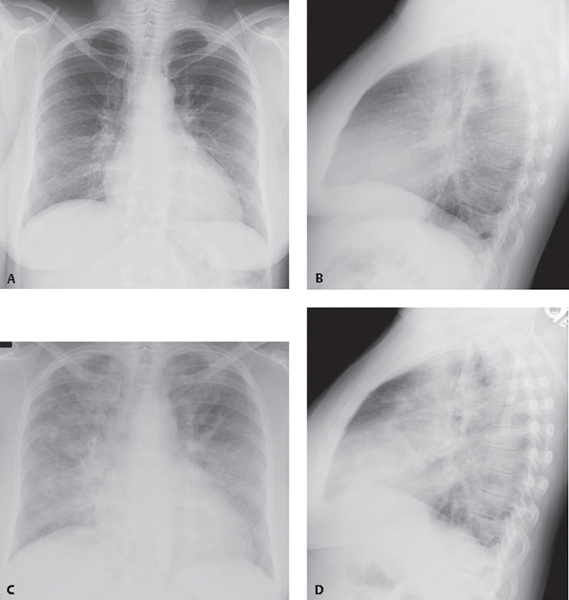
CASE 67 46-year-old woman admitted to the hospital with three-day history of progressive dyspnea, cough productive of whitish-yellow sputum, pleuritic chest pain, fever, and chills Baseline admission PA (Fig. 67.1A) and lateral (Fig. 67.1B) chest X-rays demonstrate subtle bilateral perihilar reticular opacities, right more so than left, and patchy, ill-defined consolidation in the right base paralleling the right heart border. Follow-up PA (Fig. 67.1C) and lateral (Fig. 67.1D) chest radiographs two days later reveal rapid progression of disease. Extensive ill-defined patchy and confluent consolidations are now present bilaterally. Note the absence of pleural effusion. Fig. 67.1 Influenza Pneumonia • Other Viral Pneumonias • Various Atypical Pneumonias The influenza virus is a leading respiratory pathogen that affects persons of all ages and is responsible for annual epidemics worldwide. Seasonal influenza is an acute respiratory illness that occurs primarily during winter months. Influenza pneumonia is caused by the influenza virus, an RNA virus. Three types (A, B, and C) are identified based on antigenic differences in internal proteins. Most human infections are caused by types A and B. Type A is the most virulent and can be divided into various antigenic subtypes based on the presence of two structurally, functionally, and genetically distinct surface glycoproteins: hemagglutinin (H) and neuraminidase (N). Variations of these surface glycoproteins result in evasion of pre-existing host immunity (antigenic drift) and in the emergence of viruses to which there is no pre-existing immunity (antigenic shift). Antigenic drift is responsible for annual winter outbreaks. Antigenic shift is responsible for influenza pandemics. The influenza epidemic of 1918 killed 20–40 million people and accounted for 80% of the deaths in the U.S. Army in World War I. The virus is highly contagious and transmitted from person to person via inhalation of infected airborne secretions or contact with infected secretions. The incubation period is only 24–48 hours, allowing for rapid spread of the disease. H1N1 Virus The novel swine-origin influenza type A (H1N1) virus (S-OIV), also referred to as “swine flu” by the lay press and media, and was first reported in Mexico in April 2009. Infection rapidly spread to many other countries around the world prompting the World Health Organization (WHO) to declare the emergence of a global pandemic by June 2009. As of the May 30, 2010 WHO update, more than 214 countries and overseas territories or communities reported laboratory confirmed cases of pandemic influenza H1N1 2009, including over 18,138 deaths. H1N1 is a highly contagious acute respiratory disease, spread similarly to that of seasonal influenza viruses, which includes person-to-person large-particle respiratory droplet transmission produced by coughing or sneezing or touching contaminated surfaces. The incubation period is 1–7 days. Affected patients have an acute presentation with fever, chills, prostration, myalgias, arthralgias, malaise and headache. By the end of the first week, rhinorrhea, sore throat, and dry cough develop. During the second week of illness, patients develop non-productive cough, and easy fatigability. Infection in immunocompetent patients typically follows a self-limited course. Adults with underlying chronic diseases, women in the third trimester of pregnancy and immunosuppressed patients may develop severe life-threatening pneumonia often complicated by secondary bacterial infection. Systemic complications, including Guillain-Barre syndrome, toxic shock syndrome and Reyes’ syndrome, may also occur.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Influenza Virus
Etiology
Clinical Findings
Influenza Pneumonia
H1N1
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


