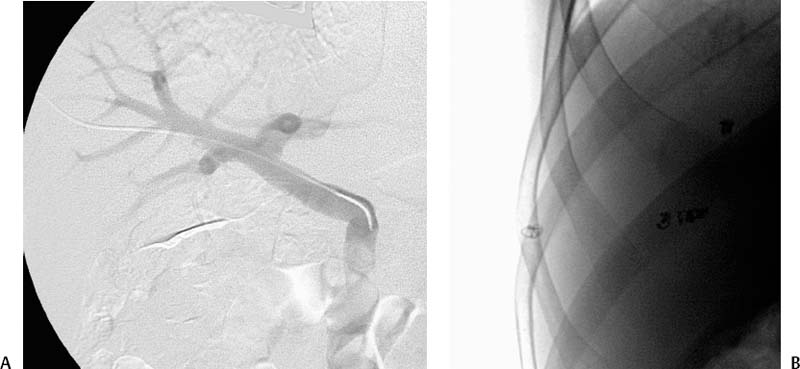
CASE 67 A 47-year-old female with brittle type I diabetes and recurrent episodes of hypoglycemic unawareness was referred to our medical center for therapy. We discuss the treatment options. Figure 67-1 Islet cell transplantation. (A) Portal venogram shows wide patency of the portal vein. The islets were transfused through the catheter into the main portal vein. (B) Final fluoroscopic image shows coil and Gelfoam (Pharmacia and Upjohn, Kalamazoo, Michigan) embolization of the transhepatic tract. A Doppler evaluation of the liver revealed wide patency of the hepatic artery, portal vein, and hepatic veins. Type I diabetes with poor glucose control. Antibacterial, antifungal, and antiviral prophylaxis was performed. The patient was brought into the interventional radiology suite. Her blood pressure, heart rate and rhythm, and oxygen saturation were monitored noninvasively. Conscious sedation was provided using fentanyl and midazolam. The anterior and right lateral abdomen was prepared using chlorhexidine solution and draped in sterile fashion. After subcutaneous administration of lidocaine, the right portal vein was punctured from a lateral approach using ultrasound and fluoroscopic guidance with a 21-gauge needle. The needle was exchanged over a 0.018-inch guidewire for a 4-French (F) Kumpe endhole catheter which was placed into the main portal vein. Portal venography was performed using iso-osmolar contrast to confirm position (Fig. 67-1A). The islet preparation was resuspended in a medium that contained 20% human albumin and heparin (35 U/kg recipient body weight if pellet volume is < 5 cc; 70 U/kg recipient body weight if pellet is 5 to 10 cc). Islets were infused via the Kumpe catheter directly into the main portal vein. The infusion was performed over about 30 minutes with portal vein pressure monitoring throughout the procedure. Portal pressure remained 12 mm Hg throughout. After the infusion, the Kumpe catheter was retracted several millimeters and the tract embolized using two 3-mm metal coils deposited just outside the portal vein entry point (Fig. 67-1B). A Gelfoam (Pharmacia and Upjohn, Kalamazoo, Michigan) plug was then positioned in the tract adjacent to the coils followed by two additional coils and an additional Gelfoam plug. The patient was observed overnight and discharged to home the next day. Anticoagulation was continued for 7 days using low-molecular-weight heparin injections.
Clinical Presentation
Radiologic Studies
Diagnosis
Treatment
Equipment
Islet Cell Transplant
Discussion
Background
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


