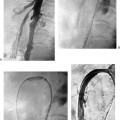
CASE 69 A 54-year-old male with new-onset hypertension underwent gadolinium-enhanced magnetic resonance angiography (MRA) of the abdomen. Figure 69-1 Gadolinium-enhanced MRA of renal artery stenosis. Coronal projection shows moderate-to-severe left renal artery stenosis. Abdominal MRA shows moderate-to-severe left renal artery stenosis (Fig. 69-1). Atherosclerotic left renal artery stenosis. The right common femoral artery was accessed using a Micropuncture set, and a 6-French (F) Balkan sheath (Cook, Indianapolis, Indiana) was inserted. A pigtail catheter was advanced into the abdominal aorta, and aortography was performed showing the left renal artery stenosis (Fig. 69-2A). Five thousand U of intra-arterial heparin were administered. Through the sheath, a 5F RC-1 catheter (Boston Scientific, Natick, Massachusetts) and 0.035-inch soft-tipped guidewire (Bentson; Boston Scientific) were used to cross the stenotic segment. Selective angiography was performed to confirm intraluminal catheter tip position and to exclude the possibility of iatrogenic dissection (Fig. 69-2B). Pressure measurements were then obtained using the 5F catheter and guiding sheath, revealing a 30 mmn Hg trans-stenotic gradient. A 0.035-inch Rosen guidewire (Cook, Bloomington, Indiana) was then positioned with its tip in the distal renal artery. A 6-mm angioplasty balloon was advanced to the site of stenosis and used to dilate the lesion. Postangioplasty angiography revealed minimal improvement in the stenosis with a residual lesion greater than 50%. The angioplasty balloon was positioned at the lesion and the sheath was advanced across the lesion. A 6- × 17-mm premounted balloon-expandable stent (Express; Boston Scientific, Natick, Massachusetts) was then advanced to the site of the lesion and “uncovered” by retracting the sheath to the ostium of the renal artery. A small amount of contrast material was injected through the sidearm of the sheath during fluoroscopy to confirm appropriate position of the stent. The balloon was inflated to expand the stent across the lesion. An angiogram was then obtained through the sheath with the guidewire remaining across the stent (Fig. 69-2C) revealing minimal residual stenosis. The trans-stenotic gradient was reduced to zero. Figure 69-2 Left renal artery stent insertion. (A) Abdominal aortogram shows left renal artery stenosis (arrow). (B) Selective distal left renal arteriogram after catheterization shows distal perfusion to the kidney. (C) Selective left renal angiogram via sidearm sheath shows alleviation of stenosis by placement of metal stent. Note guidewire in distal renal artery maintaining access across the treated lesion.
Clinical Presentation
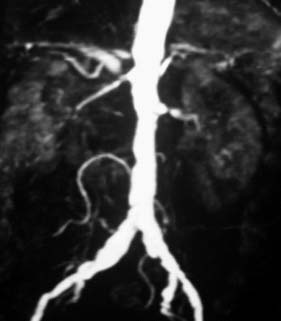
Radiologic Studies
Diagnosis
Treatment

Equipment
| Significant renal artery stenosis or stenoses Malignant, accelerated, or resistant hypertension Hypertension with unilateral small kidney Renal insufficiency with angiotensin-converting enzyme inhibition Recurrent or refractory congestive heart failure or flash pulmonary edema Rapidly declining renal insufficiency |
Discussion
Background
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


