7 Pulmonary and Systemic Veins
Introduction
Intrathoracic veins can be categorized into the systemic and pulmonary veins (PVs). The systemic veins return deoxygenated blood into the right atrium (RA) and the PVs forward the oxygenated lung blood into the left atrium (LA). Anatomical variation and congenital anomalies of these vessels are common. Knowing anatomy of these vessels is very important for correct recognition of the variants of these vessels which may have important clinical and surgical implications. Thrombosis of the brachiocephalic veins and occasionally superior vena cava (SVC) is seen after catheter insertion, a common intervention in many patients admitted to hospitals. Congenital abnormalities of the major mediastinal venous structures occur in less than 2% of people who have no other abnormalities. Although many congenital anomalies have been described, they occur with sufficient frequency without significant adverse clinical consequence: persistence of a left SVC with and without a coexisting right SVC, azygos or hemiazygos continuation of an interrupted inferior vena cava (IVC), and partial anomalous pulmonary venous return (PAPVR).
Systemic Veins
The systemic veins of the thorax include the SVC and its tributaries and the azygos system. Only the suprahepatic portion of the IVC before its entrance into the RA is located within the thorax.
Superior Vena Cava
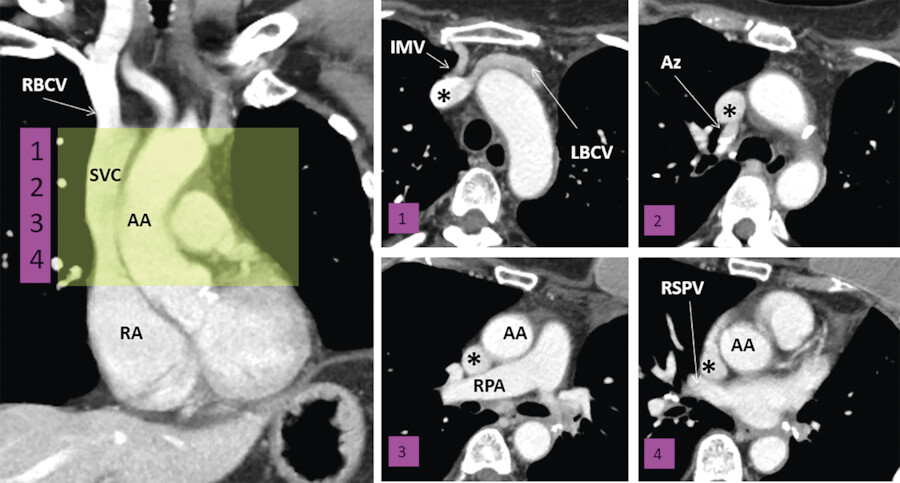
The SVC starts at the confluence of the right and left brachiocephalic veins. It travels 5 to 7 cm on the right anterior aspect of the upper mediastinum from the level of the first sternocostal junction to the superior cavoatrial junction. At the junction with the RA, the SVC is located posterolateral to the ascending aorta, anterior to the right pulmonary artery and anteromedial to the right superior PV (Fig. 7‑1). The right phrenic neurovascular bundle travels along the lateral wall of the SVC. The sinoatrial node (SA) artery encircles the SVC at the superior cavoatrial junction before entering the SA node region. The distal 2 cm of the SVC is intrapericardial and the azygos vein enters the SVC posteriorly above the pericardial reflection. Deoxygenated blood from upper extremity, head, neck, and azygos system enters the SVC. The SVC is the major conduit for passage of indwelling catheters, pacer leads, and transvenous interventional devices.
Embryology
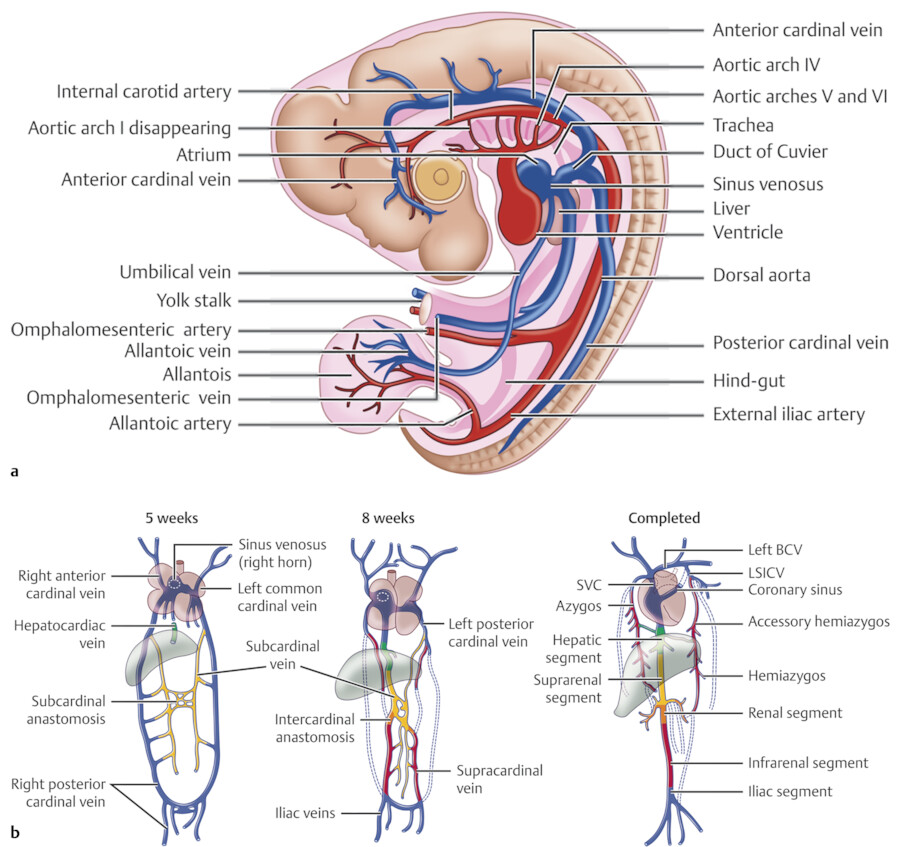
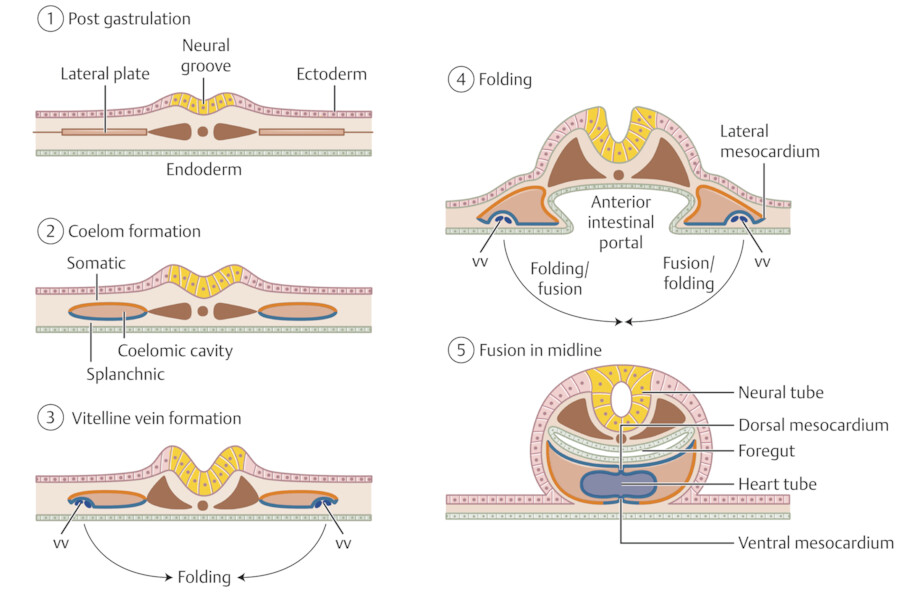
The formation and anatomical variations of the systemic venous of the thorax are the result of complex pattern in persistence and regression of the segments of three pairs of venous channels during the first 4 weeks of fetal development: (1) the omphalomesenteric (vitelline) veins, carrying blood from the yolk sac; (2) the umbilical vein, originating in the chorionic villi and carrying oxygenated blood from the placenta; and (3) the common cardinal veins (ducts of Cuvier), draining the body of the embryo. 1 , 2 , 3 , 4 , 5 , 6 All these three venous channels drain into the sinus venosus (Fig. 7‑2 a). The sinus venosus or systemic venous sinus, which connects to the right RA, is formed by myocardial differentiation of the mesenchyme that surrounds the common cardinal veins at the junction between the splanchnic and somatic mesoderm. Its opening into the RA is marked by the so-called “venous valves.”
The right and left common cardinal veins are formed by the confluence of the anterior and posterior cardinal veins 1 , 2 (Fig. 7‑2). The anterior cardinal vein drains the cephalic portion of the embryo and the posterior cardinal vein drains the remainder of its body. The left cardinal vein and terminal segment of the left vitelline vein regress during embryogenesis. The right horn of the sinus venosus further develops and eventually forms the posterior wall of the RA. The right anterior and common cardinal veins persist and form the SVC. The left horn of the sinus venosus, in conjunction with the regressing left common cardinal vein, form the coronary sinus (CS) that opens into the RA and the left anterior cardinal venous system remains as the ligament or oblique vein of the LA (vein of Marshall) draining into the CS (Fig. 7‑2). A bridging venous plexus which was formed between the right and left anterior cardinal veins around 24-mm crown-rump embryonic stage develops to be the left brachiocephalic vein. 7 The left anterior cardinal vein below this connection gradually obliterates. Its upper portion remains as part of the left superior intercostal vein (SICV). The right sinus valve persists as the valve of the IVC (Eustachian valve) and the valve of the coronary sinus (Thebesian valve). 2 The right vitelline vein forms the hepatic segment of the IVC (hepatocardiac channel) (Fig. 7‑2). Various abnormal venous connections can occur if any of these processes fails to occur properly.
Pathologies
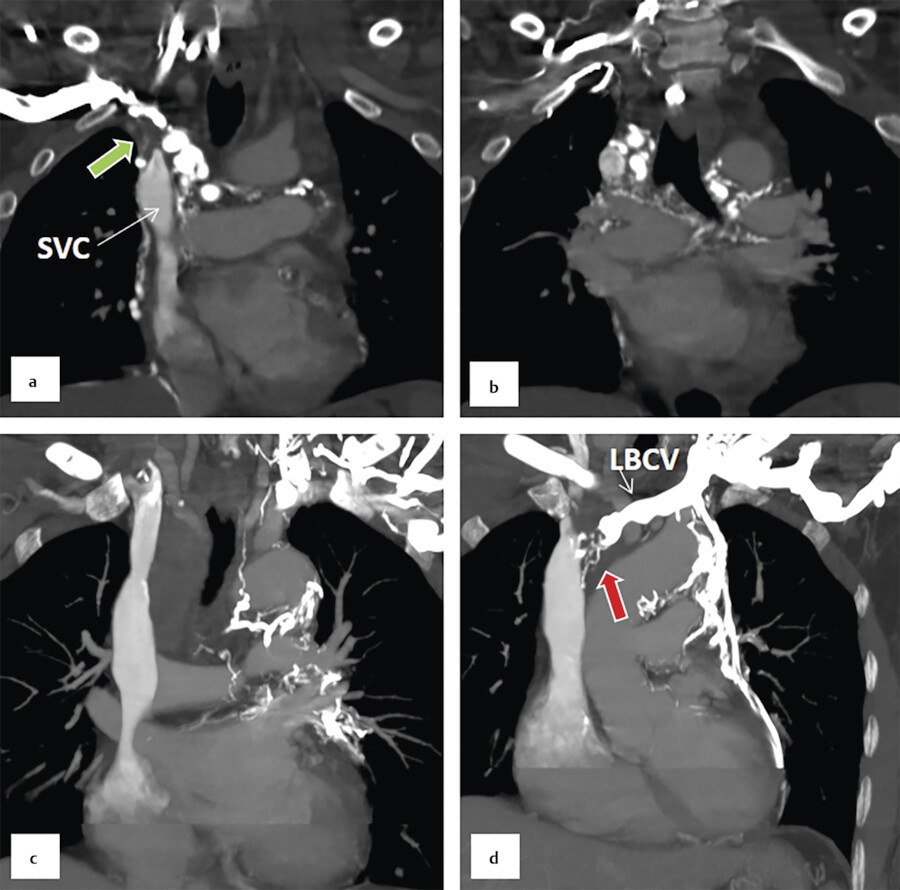
Obstruction of the SVC is usually secondary to tumor infiltrates or intrinsic thrombosis after long-term catheter insertion (Fig. 7‑3).
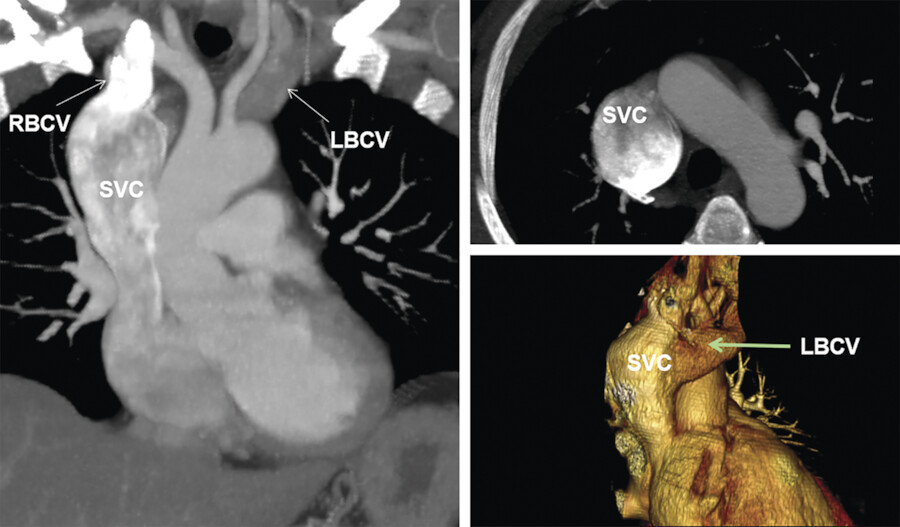
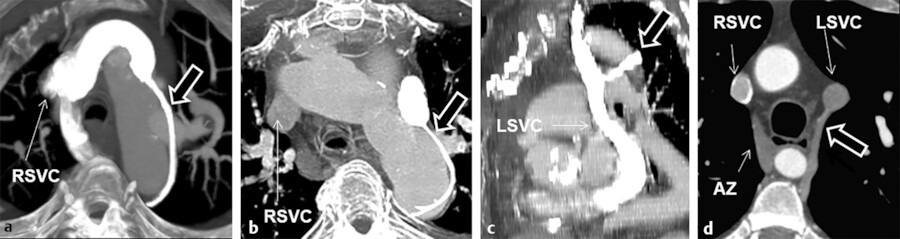
Isolated anomalies of the right SVC are rare. 8 Anomalous low insertion of the right SVC into the RA can be seen as an isolated anomaly. Congenital aneurysmal dilation of the SVC may be mistaken with a mass 9 (Fig. 7‑4). It may involve the SVC only or multiple veins in the upper mediastinum.
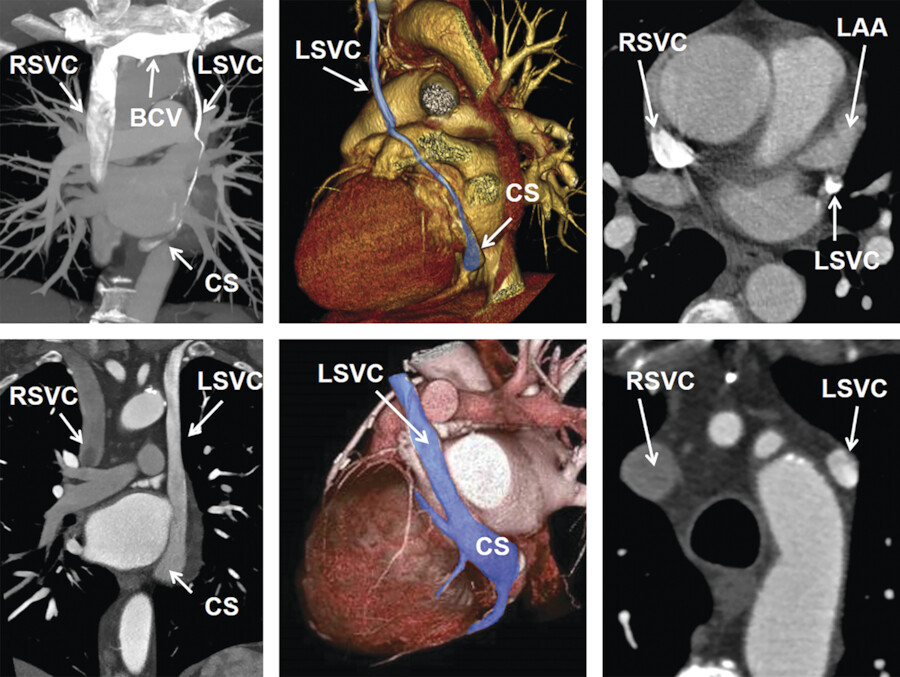
The left SVC is the most common anomalous systemic vein drainage in thorax, incidentally found in 1 out of 200 (0.5%) of computed tomography (CT) or magnetic resonance imaging (MRI) studies of chest (Fig. 7‑5). Prevalence is higher in patients with congenital heart malformation and may be seen in 5 to 10% of patients. 10 , 11 It results from failure of parts of the left anterior and common cardinal veins to regress. Isolated left SVC is less common than duplicated SVC (Fig. 7‑2). The left SVC drains the tributaries of the left subclavian and jugular veins into the coronary sinus via the oblique vein of the LA. The left SVC is closely sandwiched between the left superior PV and the left atrial appendage wall. This is a benign condition, but rarely the left SVC connects to the LA causing a right-to-left shunt.
Brachiocephalic Veins
The brachiocephalic veins are formed by the confluence of the internal jugular and subclavian veins behind the sternoclavicular joint (Fig. 7‑1). The left brachiocephalic vein passes obliquely from left to right and the right brachiocephalic vein moves downward behind the manubrium. They unite to form the SVC. The left brachiocephalic vein is longer than the right; neither has a valve. The brachiocephalic veins receive the internal thoracic and inferior thyroid veins. The left brachiocephalic vein also receives the left SICV.
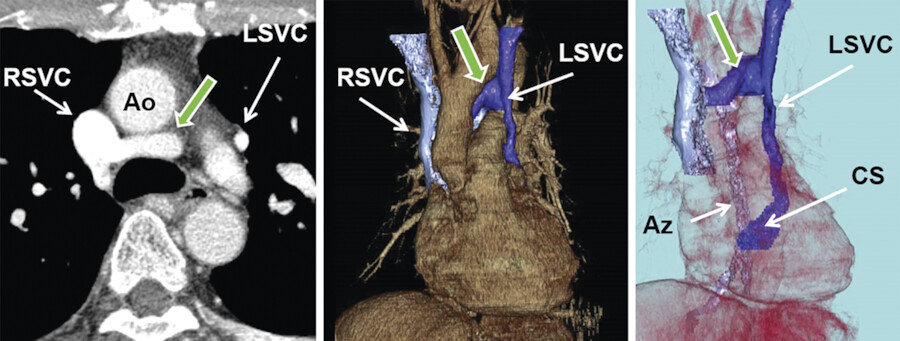
Anomalous brachiocephalic vein is uncommon, accounting for approximately 1% of congenital cardiovascular anomalies. 7 , 12 The cause of an anomalous brachiocephalic vein remains controversial and is related to abnormal regression of the anterior cardinal anastomosis. The presence of two or more (a plexus) transverse precardinal anastomoses is proposed to explain three patterns of anomalous brachiocephalic vein development: anomalous subaortic left brachiocephalic vein, persistent left SVC with a hypoplastic left brachiocephalic vein connecting to the right SVC, double SVC with agenesis of the left brachiocephalic vein, 7 and circumarctic left brachiocephalic vein (Fig. 7‑6). An anomalous subaortic left brachiocephalic vein is a benign anatomical variant. This vein, rather than joining the right brachiocephalic vein ventral to the aorta, crosses the midline dorsal to the ascending aorta to join the SVC caudal to the azygos vein (Fig. 7‑6). Recognition of the brachiocephalic vein anomalies is important to avoid misdiagnosis and prevent technical difficulty in a left arm approach for the insertion of a central venous catheter and cardiovascular intervention.
Stenosis or occlusion of the brachiocephalic vein is a common complication of long-term central venous catheter insertion (Fig. 7‑3).
Left Superior Intercostal Vein
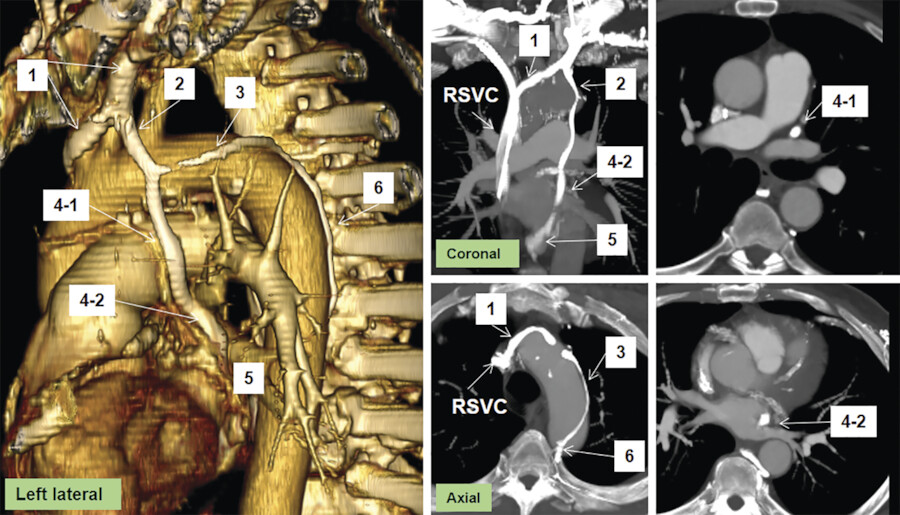
The residuals of an obliterated left anterior cardinal vein are seen as the oblique vein of the LA (Marshall) on the cardiac end and as a small vertical vein on the venous end between the left SICV and the left brachiocephalic vein 3 , 11 (Fig. 7‑7). The left SICV is a bridging vessel that links the posteriorly located azygos–hemiazygos systems with the anteriorly located left brachiocephalic vein. The left SICV drains the second, third, and fourth posterior intercostal veins, then passes forward and upward along the aortic arch to drain into the left brachiocephalic vein near the venous angle. In two-thirds, the vein connects to the accessory hemiazygos vein which is recognizable in most CT angiographies 13 , 14 (Fig. 7‑8). The left SICV is described as “aortic nipple” in up to 10% 13 of chest radiographs. Obviously, in CT scans it can be seen more frequently (45%) along the lateral side of aortic arch. This bridging venous pathway has the potential of creating a right-to-left shunt when the SVC and left brachiocephalic vein are narrowed or obstructed. In these situations, venous connections develop between the mediastinal veins or tributaries of the left SICV on the systemic side and the superior PVs (rarely the LA) on the pulmonary side. 15
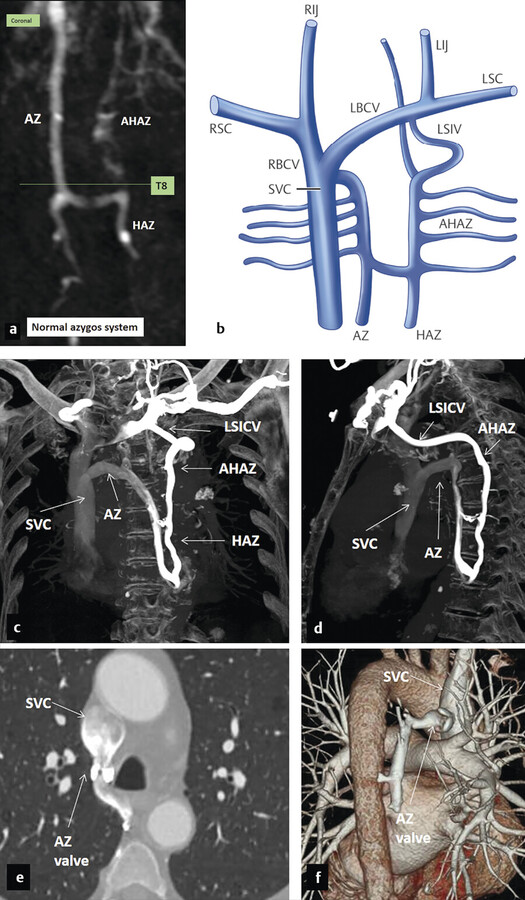
Azygos System and Inferior Vena Cava
In the thorax, the azygos system receives blood from the posterior intercostal and mediastinal venous tributaries. The SICV drains the second through the fourth intercostal spaces. The right SICV communicates with the azygos knob (Fig. 7‑9). The left SICV drains into the left brachiocephalic vein along the lateral margin of the aortic arch and may connect to the accessory hemiazygos in 70 to 80% of cases. The azygos vein drains into the SVC just cephalad to the right main bronchus. In many cases, a valve exists at the confluence of the azygos vein with the SVC (Fig. 7‑9). The hemiazygos vein crosses midline at T8 to T9 level and behind the descending thoracic aorta to join the azygos vein (Fig. 7‑9). From this point, the accessory hemiazygos vein extends further cephalad in a left paravertebral position and communicate with the azygos and paravertebral veins at different levels.
Embryology
During the fourth to sixth weeks of embryological development, a pair of posterior cardinal veins drain all but the cephalic portion of the embryo. 11 , 16 , 17 Later at the sixth week, a second new pair of vein, the subcardinal veins, develop which become dominant at seventh weeks while most of the posterior cardinal veins gradually disappear (Fig. 7‑2). Important anastomoses develop between the right and left subcardinal veins anterior to the aorta. The right subcardinal vein further develops to the renal and suprarenal portions of the IVC which connect with the hepatic segment of the IVC (derived from the termination of the right omphalomesenteric vein). At the eighth week, the posterior cardinal veins will be replaced proximally by a third pair of veins, the supracardinal veins, which develop medial and dorsal to the posterior cardinal veins and later anastomose each other behind the aorta. The azygos vein derives mainly from the upper right supracardinal vein, but the azygos arch seems to originate from the remaining of the upper cranial segment of the right posterior cardinal vein. Similarly, upper left supracardinal vein turns into the hemiazygos vein and residual of the cranial segment of the left posterior cardinal vein may form the posterior portion of left SICV. The IVC development is complex and five embryological segments contribute to its composition. In caudal–cranial order, these segments include posterior cardinal veins (iliac segment); right supracardinal vein (infrarenal segment); anastomosis between the right supra- and subcardinal veins (renal segment); right subcardinal vein (suprarenal segment); and hepatocardiac canal (hepatic segment).
Variants and Pathologies
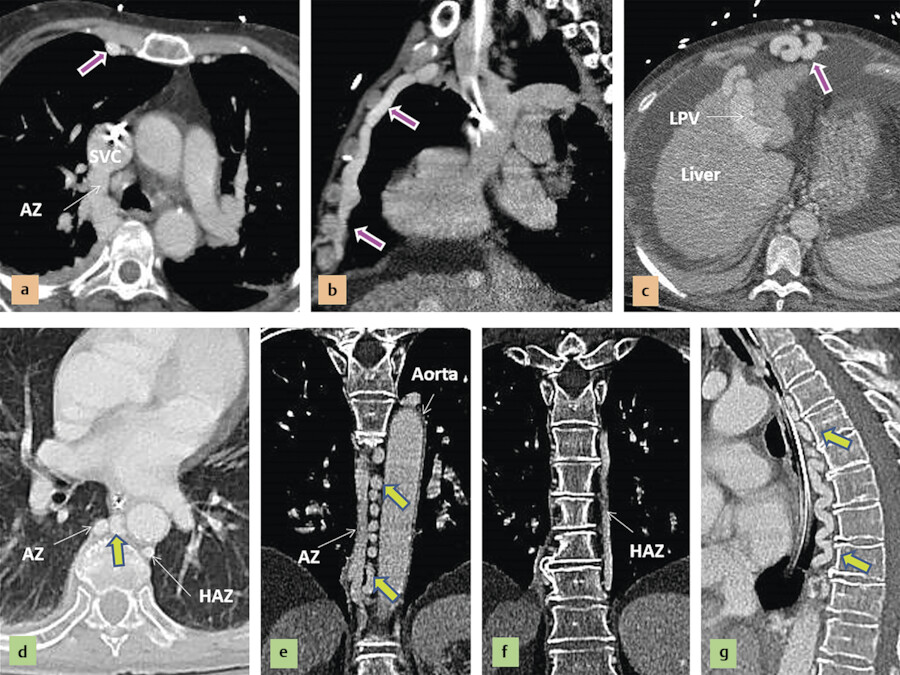
Dilation of the azygos system is a common finding in patients with obstruction of the SVC, acting as collateral pathway to direct blood into the LA. Azygos will also be dilated in cirrhosis due to abnormal portosystemic shunting (Fig. 7‑10).
Azygos and Hemiazygos Continuation of the IVC
Abnormal connection of the hepatic segment to the suprarenal segment of the IVC results in azygos or hemiazygos continuation of the venous system from abdomen into the thorax 16 (Fig. 7‑11). Therefore, although a large azygos or hemiazygos vein is the predominant finding in these venous anomalies, the primary anomaly is the IVC maldevelopment. These anomalies may be isolated or associated with other anomalies. It can be part of situs anomalies with left isomerism (polysplenia syndrome), in which the liver and stomach are located in midline, multiple spleens are found along the greater curvature of the stomach, and the minor fissure of the right lung is absent. 18 Azygos continuation is rare in patients with asplenia (right isomerism).
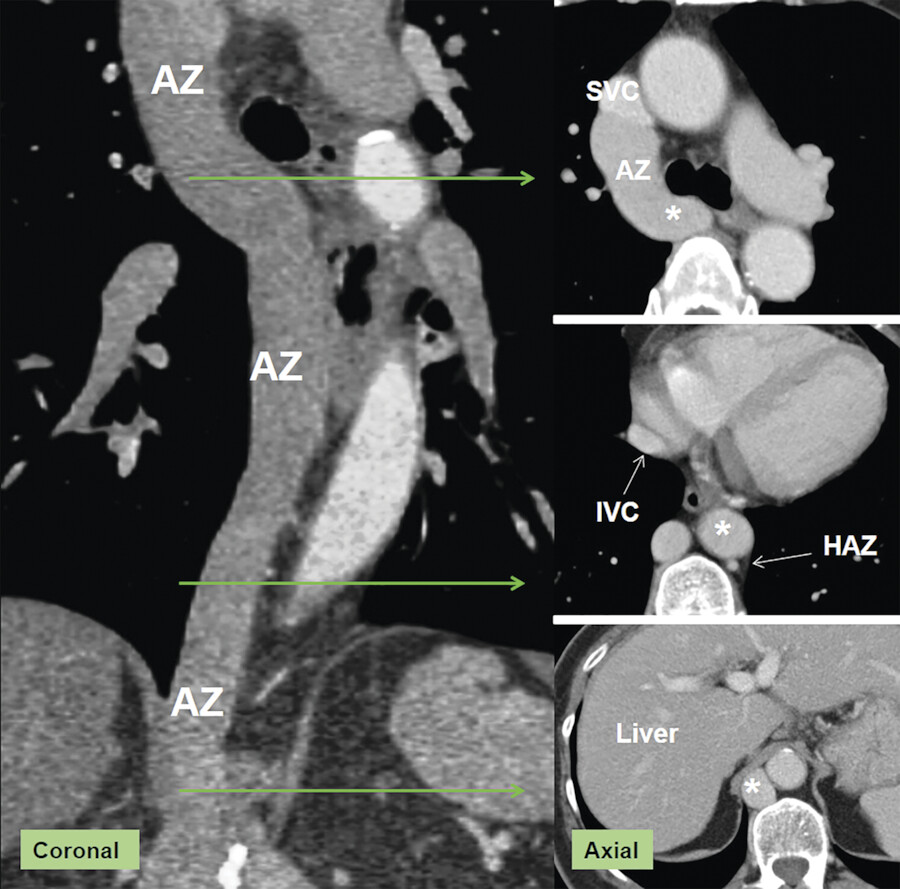
The imaging features of azygos continuation of the IVC include dilation of the azygos vein, azygos arch, and SVC caused by increased flow. The hepatic veins drain into the RA via the suprahepatic IVC (Fig. 7‑11). The hepatic segment of the IVC is absent or hypoplastic, and this condition must be documented to exclude other causes of an enlarged azygos vein. Hemiazygos continuation of a left-sided IVC is a rare anomaly in which a dilated hemiazygos vein drains into the azygos vein at T8 to T9. Alternatively, the hemiazygos vein continues cephalad to connect with the accessory hemiazygos vein and a left SVC, all of which are dilated.
Other Variants or Anomalies of the Azygos Vein
Azygos lobe of the right lung apex occurs in 1% of population as a result of malposition of terminal part of the azygos vein. 19 It occurs when the right posterior cardinal vein, one of the precursors of the azygos vein, fails to migrate over the apex of the lung and penetrates it instead, carrying along pleural layers that entrap a portion of the right upper lobe. This is a benign anatomical variant and should not be mistaken with major anomalies. Left azygos lobe is rare and is caused by a malpositioned left SICV draining into the left brachiocephalic vein. 20
In rare occasions, the azygos vein enters the right brachiocephalic vein, right subclavian vein, intrapericardial SVC, or RA. Total absence of the azygos vein, a very rare anomaly, arises when the cranial segment of the right supracardinal vein fails to develop. 21 It is usually asymptomatic. Normal drainage of the right and left intercostal veins by the hemiazygos and accessory hemiazygos veins will be compromised causing unusual enlargement of these veins.
Pulmonary Veins
Anatomy
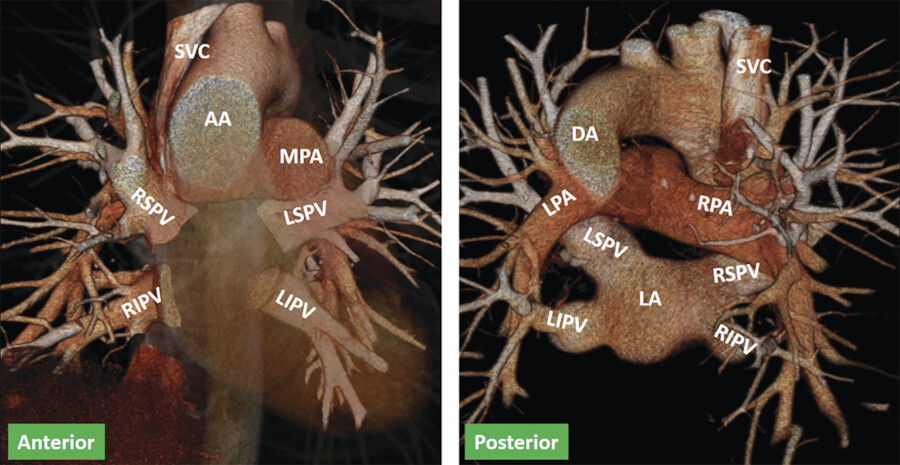
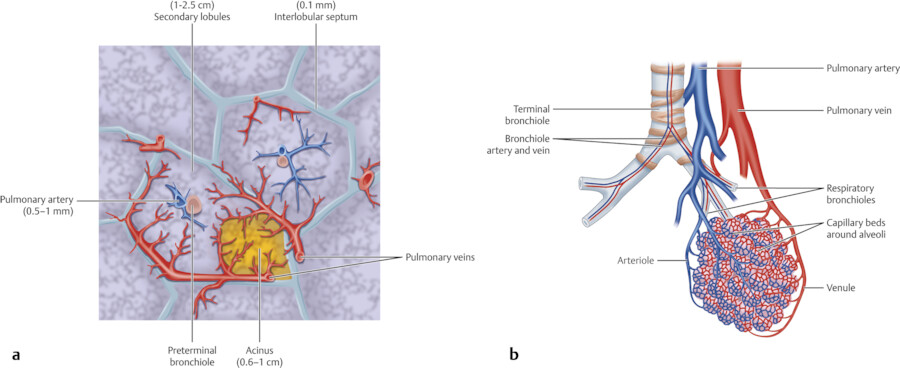
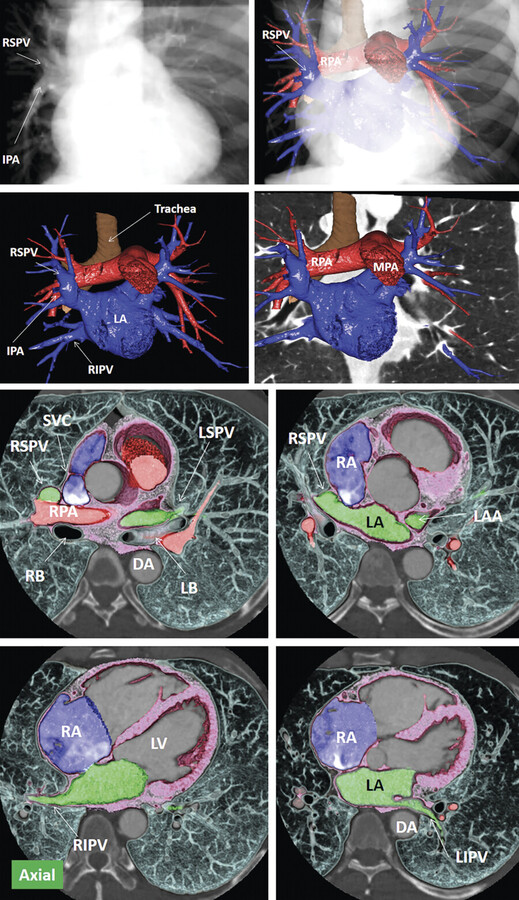
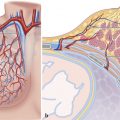
Normal PV anatomy consists of two right-sided and two left-sided veins with separate ostia (Fig. 7‑12). The pulmonary venous system carries oxygenated blood from capillaries toward the LA. The capillaries arise from the branching arterioles, which then form a network of vessels in the wall of alveoli (Fig. 7‑13). These capillaries have very thin walls, less than 0.1 µm thick, permitting gas exchange and oxygenation of blood. Arteriovenous shunting can occur normally near the terminal bronchioles that let passage of small particles less than 500 μm. 22
The pulmonary venules run in the interlobular septa, between lung segments, in the visceral pleura, and along the interlobar fissures (Fig. 7‑13). Segmental tributaries coalesce to form lobar veins.
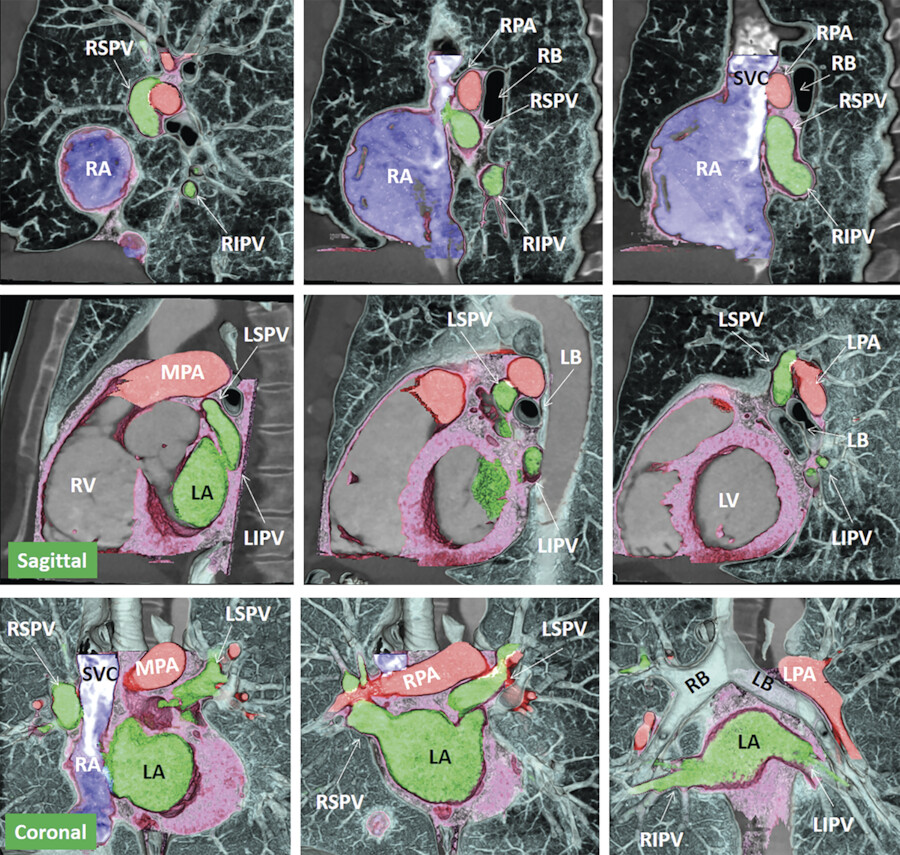
The anatomy and size of the LA and PVs are commonly variable. The superior PVs typically drain the upper and middle lung lobes, whereas the inferior PVs originate from the lower lobes (Fig. 7‑14). The right superior PV has a vertical course, initially passing along the lateral side of the SVC and anterior to the right pulmonary artery and then behind the superior cavoatrial junction and inferior to the right pulmonary artery before entering the LA. In contrast, the left superior PV has a more horizontal course superior and then anterior to the left mainstem bronchus and inferior to the main pulmonary artery before connecting to the LA. The inferior PV courses horizontally in the lower hemithorax. The left inferior PV passes anterior to the descending aorta and medial to the left lower lobe bronchus before reaching the LA. Its ostium may lie anterior to the esophagus.
Embryology
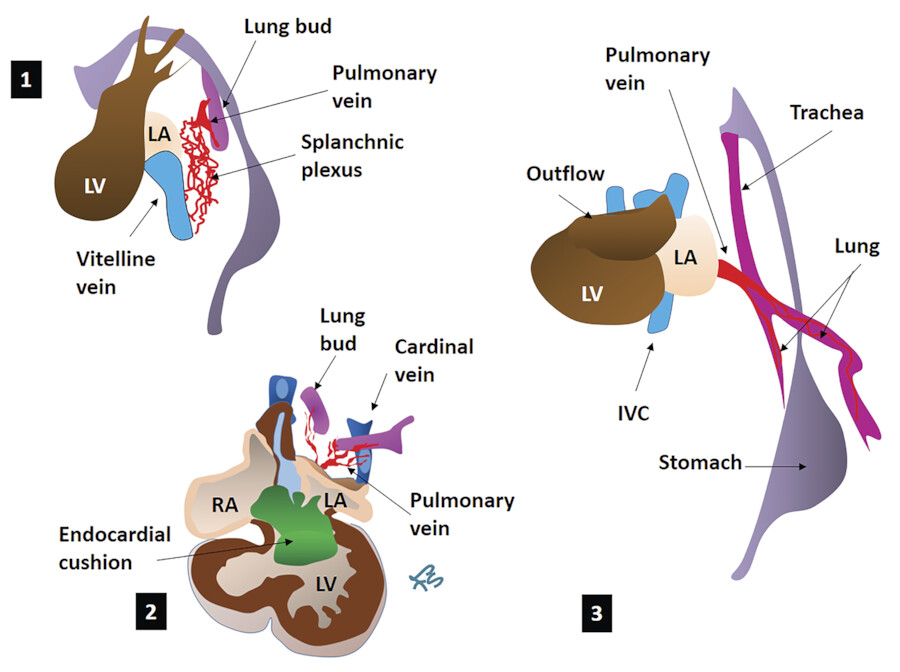
The primary heart tube is formed from fusion of vitelline veins which differentiate into myocardium (Fig. 7‑14). The vitelline veins also fuse to form the portal vein. Later, development of other systemic venous systems including the cardinal and the umbilical venous systems occurs. Together with the umbilical veins, the portal vein contributes to the hepatic vascular bed. The PVs are the fourth venous system that becomes connected to the primary heart. In contrast to the SVC and coronary sinus which arise from the sinus venosus, the PV does not originate from the primary myocardium surrounding the orifices of the systemic venous tributaries. It derives from the splanchnic mesoderm that overlies the foregut and their development is closely related to the development of the lung buds 5 (Fig. 7‑16. During the first 2 months in utero, the lung buds develop from the foregut. Blood returning from the lung buds initially drains into the splanchnic plexus. The splanchnic venous plexus which extends from the heart to the liver communicates with the paired cardinal veins as well as the umbilicovitelline veins. Within the mediastinal splanchnic mesoderm, a midpharyngeal strand vascular plexus canalizes to form the primitive PV. This primitive common PV connects the lung venous network to the LA close to the atrioventricular junction where the primary dorsal mesocardium was connected. 23 , 24 Later, the pulmonary venous connections to the cardinal and umbilicovitelline veins disappear. 24 Along with growth of the primary atrial septum on the right side of the pulmonary venous orifice, final location of the PV orifice is determined within the morphologically LA. Four pulmonary venous tributaries of the primitive PV subsequently develop and assimilate into the LA.
Various abnormal systemic or pulmonary venous connections develop if any of these processes fails to occur properly. 25 If the common PV fails to properly incorporate into the posterior left atrial wall, PV stenosis/atresia or cor triatriatum will occur. 24 Anomalous PV return is total if the entire PV return is directed to the RA and partial if only a portion of the PV circulation is affected. The proportion of anomalous PV return influences the extent of physiological blood flow compromise and the age of presentation. In general, the sites of anomalous connections are divided into (1) direct right atrial wall; (2) the derivatives of the right common cardinal systems including the SVC and azygos vein; (3) the derivatives of the left common cardinal system, specifically the coronary sinus; and (4) the derivatives of the umbilicovitelline system such the portal vein. 23 Abnormal opening of the right superior PV at right superior cavoatrial junction results in a sinus venosus type of atrial septal defect (ASD).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


