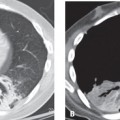
CASE 70 33-year-old man with three- to four-day history of dyspnea, non-productive cough, fevers, and chills admitted to the hospital with presumptive diagnosis of community-acquired pneumonia. Antibiotic therapy was initiated without improvement. He developed progressive hypoxia. CTPA for pulmonary embolism on hospital day 4 revealed no embolism. Two days later, ARDS ensued. Admission PA (Fig. 70.1A) chest X-ray shows bilateral, perihilar, segmental ground glass and air space consolidations. Follow-up AP portable chest exam three days later (Fig. 70.1B) reveals significant progression of disease. Chest CT (lung window) (Figs. 70.1C, 70.1D, 70.1E, 70.1F) acquired on hospital day 4 demonstrates a patchy pattern of variable attenuation characterized by foci of ground glass, consolidation, hypoattenuated lung with reduced perfusion, and intervening areas of normal lung. The combination of “mixed densities” throughout the lung gives it a geographic appearance similar to a preserved meat product called head cheese or hog’s head cheese (Fig. 70.2) and it is therefore referred to as the head cheese sign. Mycoplasma Pneumonia • Typical Bacterial Pneumonias • Other Atypical Pneumonias • Viral Pulmonary Infection • Hypersensitivity Pneumonitis • Acute Interstitial Pneumonia (AIP) Mycoplasma is considered an “atypical” bacterium; it lacks a cell wall and produces pulmonary infection through extracellular growth and interference with ciliary function. It is a common cause of community-acquired pneumonia and is probably responsible for approximately 20–30% of the pneumonias that affect the general population. Infections occur year-round, but typically in the fall and winter months. The incidence of M. pneumoniae infection in the United States is approximately 1/1,000 persons. Epidemics of Mycoplasma pneumonia occur every 4–8 years in the general population and are more frequent within closed populations (e.g., college dorms, military barracks, and prisons). Mycoplasma pneumonia is caused by the organism Mycoplasma pneumoniae
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


