8 Pediatrics
Approach and Analysis
A number of emergent conditions are unique to the pediatric and neonatal age groups, and these are addressed in this chapter. Conditions also seen in adults, such as intussusception and appendicitis, can be found in the corresponding chapters organized by anatomy.
Studies that do not utilize ionizing radiation are preferred in the pediatric age group. Because the lifetime risk of developing a radiation-induced cancer is greater with early exposure, it is prudent to avoid unnecessary X-ray and CT examinations in children and to minimize radiation dose in any necessary study that utilizes ionizing radiation. Fortunately, most practices and equipment manufacturers have protocols and techniques that reduce radiation dose to the minimum needed for accurate diagnosis. Ultrasound and MRI are preferred for cross-sectional imaging, especially in the diagnosis of pediatric abdominal pain and in the often-repeated evaluation of hydro-cephalus in children with ventriculoperitoneal shunts.
In children with suspected appendicitis, ovarian torsion, testicular torsion, intussusception, or pyloric stenosis, ultrasound should be attempted prior to CT. Radio-graphs are the primary imaging modality for acute thoracic disease, ingested foreign bodies, and musculoskeletal injuries, and they can be helpful in evaluating abdominal pain by establishing the diagnosis of severe constipation as well as bowel obstruction. In the emergency setting, CT is generally reserved for significant traumatic injury and for acute abdominal pain that cannot be diagnosed by clinical and laboratory findings, plain radiography, and ultrasound.
Imaging and Anatomy
Skeletal Survey for Nonaccidental Trauma
Indications: Suspected child abuse.
– AP/lateral skull
– AP/lateral cervical and lumbar spine
– AP/lateral thorax and abdomen
– AP humeri, forearm, hand, femora, tibiae and fibulae, and feet
CT—Abdomen
Indications: Appendicitis, acute abdomen.
Technique: ~ 175 mA, 120 kV
Oral contrast: Dilute Gastrografin (up to 1 liter depending on age and size)
IV contrast: 1.5 mL/kg at 3 mL/sec, 90-second delay (symphysis to pubis)
Images: 5-mm axial, 0.6-mm reconstruction, 3-mm coronal and sagittal reformation
Approximate radiation dose: 400 mGy
Ultrasound—Generalized Abdominal Pain
Indications: Pain, mass, hernia.
Probe: Linear probe (9 MHz for infants, curved 6 MHz for older children)
Views:
– Liver—longitudinal and transverse
– Porta hepatis—main portal vein and common bile duct
– Pancreas/aorta/superior mesenteric artery—midline transverse
– Hepatorenal space (demonstrate lack of free fluid)
– Kidneys—longitudinal and transverse (measure length)
– Spleen—longitudinal and transverse (measure maximal length)
– Bladder—midline longitudinal and transverse (demonstrate lack of extravesical free fluid)
– Lymph nodes—mesenteric, right lower quadrant, and periaortic
Ultrasound—Suspected Appendicitis
Indications: Right lower quadrant pain.
Probe: Linear probe (12 MHz or 9 MHz depending on body habitus)
Views:
– Right psoas muscle—transverse including iliac artery and vein (± color Doppler
– Cecum and terminal ileum—longitudinal and transverse
– Region of appendix—transverse of region of appendix (± color Doppler)
– Bladder—midline longitudinal and transverse (show lack of extravesical free fluid)
– Right kidney—longitudinal and transverse
Abnormal appendix:
– Measure greatest diameter, color Doppler to show hyperemia
– Hepatorenal space (demonstrate lack of free fluid)
No appendicitis/appendix not seen:
– Right kidney (exclude stone or hydronephrosis)
– Gallbladder
– Ovaries (in girls) document volume and color flow
– Adnexal region if ovaries are not seen
Ultrasound—Suspected Intussusception
Indications: Abdominal pain.
Probe: 12 MHz linear probe (9 MHz may be used for evaluating the right kidney and hepatic flexure)
Views:
– Transverse images of colon—cecum, ascending, hepatic flexure, transverse, splenic flexure, and descending
– Mesenteric, right lower quadrant, and periaortic lymph nodes should be measured if identified
– Right kidney—longitudinal and transverse
– Hepatorenal space (demonstrate lack of free fluid)
– If an intussusception is identified, evaluate flow with color Doppler
– Identify any free or loculated peritoneal fluid
Ultrasound—Suspected Hypertrophic Pyloric Stenosis (HPS)
Indications: Projectile vomiting in young infant.
Probe: 12 MHz linear probe. Patient should be scanned supine and in right posterior oblique positions. It may be necessary to fill the stomach with a small amount of water if gastric air prevents visualization of the antrum
Views:
– Midline transverse images of pancreas/aorta/superior mesenteric artery
– Pylorus—image maximal canal length (normal is less than 17 mm), image maximal wall thickness from outer wall to mucosa (normal is less than 3 mm). Pyloric thickening should be fixed in HPS. If mobile, consider pylorospasm.
Ultrasound—Testicular or Appendix Testis Torsion
Indications: Scrotal pain.
Probe: Linear probe (12 MHz or higher)
Views:
– Three transverse views of both testes on one image (upper, lower, mid)
– Three longitudinal views of each testicle
– Color and arterial flow Doppler both testes (longitudinal and transverse)
– Epididymis (longitudinal and transverse ± color Doppler)
– Document hydrocele if present
– Measure testicular dimensions
Salter-Harris Classification of Pediatric Fractures
Salter-Harris classification of pediatric fractures is seen in Fig. 8.1.

Clinical Presentations and Differential Diagnosis
Clinical Presentations and Appropriate Initial Studies
Cough and Dyspnea
Chest X-ray
– Bronchiolitis/reactive airway disease (young children)
– Pneumonia
– Congenital cardiac disease
– Tracheoesophageal fistula (newborns)
Vomiting in the Newborn
Abdominal plain radiograph
Ultrasound
– Duodenal or other small-bowel atresia
– Midgut volvulus/malrotation
– Pyloric stenosis
Abdominal Pain
Ultrasound
CT or MRI may be necessary if ultrasound not diagnostic
– Appendicitis
– Testicular or ovarian torsion
– Intussusception
– Colitis
Hip Pain
Pelvis plain radiograph
Ultrasound
MRI for evaluation of osteomyelitis and bone tumors
– Septic arthritis
– Toxic synovitis
– Osteomyelitis
– Eosinophilic granuloma
– Slipped capital femoral epiphysis
– Avascular necrosis
– Legg-Calvé-Perthes disease
– Juvenile rheumatoid arthritis
– Ewing sarcoma
– Osteoid osteoma
Differential Diagnosis
Supratentorial Brain Tumors
Astrocytoma
Primitive neuroectodermal tumor (PNET)
Choroid plexus papilloma (lateral ventricle)
Pineal tumors
Infratentorial Brain Tumors
Juvenile pilocytic astrocytoma
Brainstem glioma (fibrillary astrocytoma)
Medulloblastoma (fourth ventricle)
Ependymoma (fourth ventricle)
Suprasellar/Parasellar Mass
Craniopharyngioma
Optic glioma
Germinoma
Supraglottic Narrowing
Croup
Epiglottitis
Retropharyngeal abscess
Pulmonary Mass
Metastatic tumor (osteosarcoma, Wilms, neuroblastoma)
“Round” pneumonia
Focal Pulmonary Opacity in Newborn
Pulmonary sequestration
Bronchogenic cyst
Congenital cystic adenomatoid malformation
Lucent or Cystic Pulmonary Lesion in Newborn
Congenital lobar emphysema
Cystic adenomatoid malformation
Diaphragmatic hernia
Mediastinal Mass
Normal thymus (< 2 yrs)
Lymphoma
Germ cell tumor
Bronchogenic or enteric cyst
Adenopathy
Neuroblastoma (posterior mediastinum)
Abdominal Mass
Neuroblastoma
Hepatoblastoma
Wilms tumor
Appendiceal abscess
Rhabdomyosarcoma
Intestinal Obstruction in Newborn
Duodenal atresia/stenosis/web
Annular pancreas
Jejunal atresia
Meconium plug syndrome/meconium ileus
Ileal or anal atresia
Hirschsprung disease
Intestinal Obstruction in a Child
Intussusception
Incarcerated inguinal hernia
Adhesions
Appendicitis
Malrotation/volvulus
Meckel diverticulum
Right Lower Quadrant Mass in a Child
Appendicitis
Intussusception
Duplication cyst
Aggressive Bone Lesion in a Child/Adolescent
Osteosarcoma
Ewing sarcoma
Osteomyelitis
Eosinophilic granuloma
Neuroblastoma metastasis
Leukemia/lymphoma
Nonaccidental Trauma
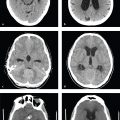
Children who suffer nonaccidental trauma (NAT) are often brought to the emergency department with minor rather than catastrophic injuries. Emergency physicians and radiologists are therefore in a unique position to first identify NAT, and recognition of characteristic injury patterns can potentially avert future abuse or neglect. Common injuries include fractures, intracranial hemorrhage or contusion, and intra-abdominal injuries. Head injury is important to recognize, because it represents a frequent cause of death in abused children below the age of 3.
Suspicious injuries include any fracture in a preambulatory child, any injury incompatible with the clinical history, unusual delay in seeking medical attention, retinal hemorrhage, multiple fractures in the absence of any family history of osteogenesis imperfecta, and subdural hematomas of different ages. A skeletal survey should be performed in cases of suspected abuse to evaluate the location and extent of present and remote osseous injuries.
Certain fractures have been recognized as indicative of NAT: metaphyseal (bucket-handle or corner) fractures, posterior rib fractures, skull fractures, scapular fractures, and sternal fractures. Periosteal reactions and juxtaosseous soft tissue calcifications signify healing fractures and should be carefully documented for medicolegal purposes.
Head CT may identify skull fractures missed by skeletal survey as well as more significant brain injury. Nonparietal skull fractures, diastatic sutures, cross sutures, or depressed fractures should be considered suspicious. MRI can evaluate the brain parenchyma more sensitively and show subdural hematomas of varying ages, hypoxic-ischemic injury, cerebral contusions, and traumatic subarachnoid hemorrhages ( Fig. 8.2 ).

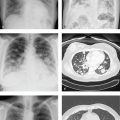
Lung Disease of Prematurity
Lung disease of prematurity, also known as respiratory distress syndrome (RDS), is an acute lung disease seen in children born before the lungs produce adequate surfactant to maintain alveolar expansion. It is seen in neonates younger than 32 weeks gestational age or who weigh less than 1,200 grams. Symptoms, which are usually evident within hours of delivery, include tachypnea, expiratory grunting, nasal flaring, and substernal and intercostal retractions. In addition to prematurity, other risk factors include maternal gestational diabetes, prenatal asphyxia, and multiple gestations.
Radiographs show a bell-shaped thoracic contour. The lung parenchyma has a fine granular, or “ground glass,” appearance, often with air bronchograms.
Complications of RDS are related to ventilation and barotrauma and include pulmonary interstitial emphysema, pneumothorax, and bronchopulmonary dysplasia.
Treatment consists of administration of artificial pulmonary surfactant and supportive ventilation and oxygen therapy. With the increased use of antenatal steroids to accelerate pulmonary maturity, the incidence and severity of hyaline membrane disease has been declining ( Fig. 8.3 ).

Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


