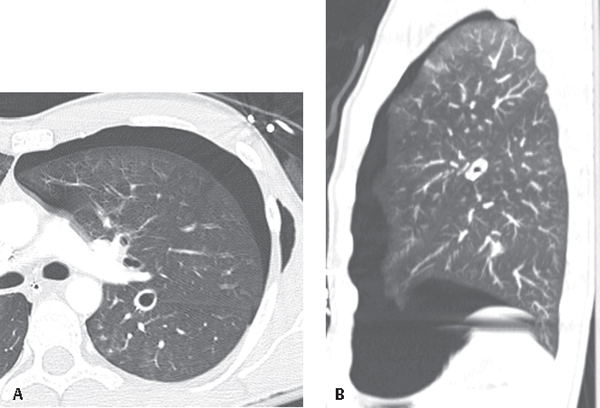
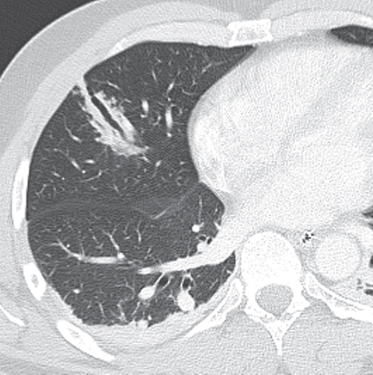
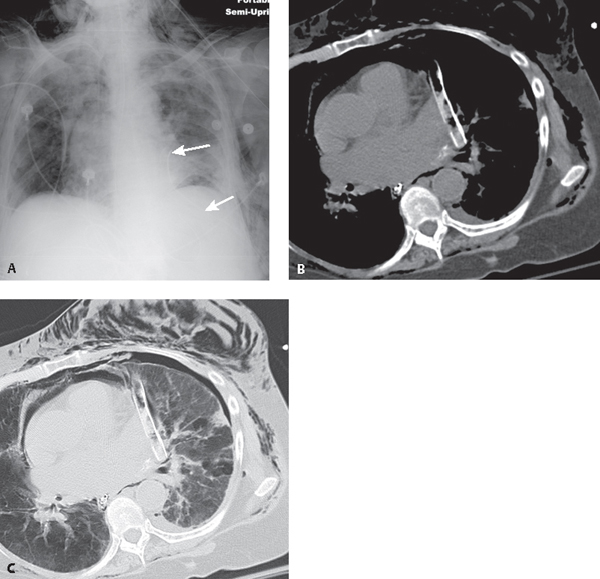
CASE 85 Series of five different unrelated trauma patients who share in common placement of pleural thoracostomy tubes in anomalous clinically undesirable but unsuspected locations Malpositioned thoracostomy tubes (Figs. 85.1, 85.2, 85.3, 85.4, 85.5). Axial (Fig. 85.1A) and accompanying sagittal MIP (Fig. 85.1B) chest CTs (lung window) show intrafissural placement of the left pleural drain in the oblique fissure. Note the persistent, inadequately decompressed pneumothorax. Axial CT (Fig. 85.2) (lung window) reveals intraparenchymal placement of the right chest tube. The anterior-placed pleural drain pierces the right middle lobe. Note the intraparenchymal hemorrhage along the course of the pleural drain. AP chest X-ray (Fig. 85.3A) demonstrates a left inferomedial pleural drain overlying the left heart. There is a persistent left subpulmonic pneumothorax, pneumomediastinum, and extensive subcutaneous air in the chest wall bilaterally. Accompanying axial CT images (Fig. 85.3B, mediastinal window; and Fig. 85.3C, lung window) confirm mediastinal placement of the left pleural drain. Note the chest tube relationship to the left atrial appendage. Coned-down frontal chest X-ray (Fig. 85.4) shows three extrapleural thoracostomy tubes inappropriately positioned in the subcutaneous tissues of the chest wall. Note the persistent hydropneumothorax and air space disease. CT topogram (Fig. 85.5A) demonstrates a kinked right chest tube and a subdiaphragmatic left chest tube. Note its relationship to the ipsilateral diaphragm. Axial CT (mediastinal window) (Fig. 85.5B) confirms subdiaphragmatic placement of the chest tube insinuated between the stomach and the splenic hilum. Fig. 85.1 Fig. 85.2 Fig. 85.3
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


85 Malpositioned Thoracostomy Tubes




