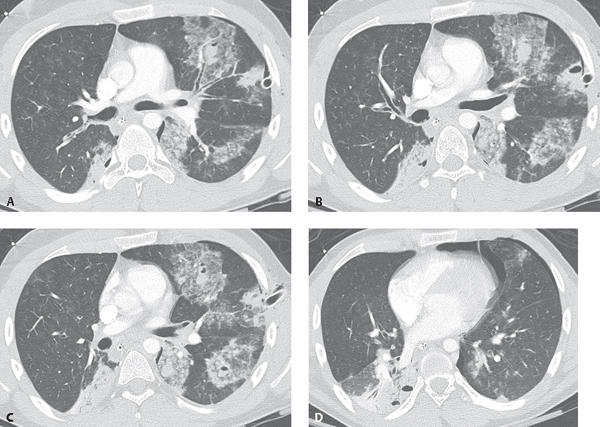
CASE 89 Young construction worker who fell 25 feet from a platform. Type 1 laceration with hematopneumocele, anterior segment left upper lobe. More laterally a contusion parallels the chest tube. Contusions in the left lower lobe and a contusion with Type 2 laceration, superior segment right lower lobe (Fig. 89.1A). Pulmonary contusion with intraparenchymal hematoma, left upper lobe. Contusion with Type 3 laceration, left upper lobe. and Type 2 laceration, superior segment right lower lobe (Fig. 89.1B). Pulmonary contusions with Type 1 lacerations with hematopneumocele in the lingula and left lower lobe. Contusion with an intraparenchymal hematoma also parallels the thoracic spine in the left lower lobe (Fig. 89.1C). Type 2 lacerations in the posterobasal segment right lower lobe and contusions in the posterobasal segment left lower lobe and lingula (Fig. 89.1D). A residual left pneumothorax is present Fig. 89.1 (Images courtesy of Janae Johnson, MD, VCU Medical Center, Richmond, Virginia.) Multifocal Pulmonary Lacerations and Contusions None Pulmonary lacerations represent serious sequelae of chest trauma characterized by disruption of normal lung architecture, unlike pulmonary contusions, and are therefore a potentially more serious lung injury. Lacerations may be caused by perforation of the lung parenchyma or pleura (e.g., stab wounds, gunshot wounds, and rib fractures) or by inertial deceleration. As with contusions, pulmonary lacerations usually occur near solid structures in the chest such as the ribs or thoracic spine. Pulmonary lacerations are classified into four categories based upon the nature of the applied force and the CT appearance. Type I
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Pulmonary Lacerations
Etiology
![]()
Stay updated, free articles. Join our Telegram channel





Full access? Get Clinical Tree


