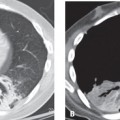
CASE 91 26-year-old man involved in a MVC with vehicular ejection Axial (Fig. 91.1A) and coronal MIP (Fig. 91.1B) chest CT (lung window) shows a right main bronchus injury and a fallen lung sign. Note the caliber change in the right main bronchus relative to the left, persistence of a large right pneumothorax despite chest tube placement, and lateral-inferior collapse of the detached right lung away from its hilum. Tracheobronchial Injury with Fallen Lung Sign None Injuries of the tracheobronchial tree are relatively rare, but may occur with blunt or penetrating trauma, and with iatrogenic injuries resulting from traumatic intubation or over-inflation of an ET tube balloon cuff or tracheostomy placement. The incidence is estimated at 2% in blunt chest and neck trauma and 1–2% in penetrating chest trauma. Laryngotracheal injuries occur in 8% of patients with penetrating neck injuries. Bronchial injuries are more common than tracheal injuries, and more than 80% occur within 2 cm of the carina. Right-sided bronchial injuries are also more common than left-sided injuries. Those bronchial injuries within the pleural envelop (i.e., distal to insertion of the pulmonary ligament) more likely result in an ipsilateral pneumothorax, whereas those occurring outside the pleural envelop (i.e., medial to the pulmonary ligament) are associated with pneumomediastinum. Additionally, because the left main bronchus has a longer mediastinal course than the right main bronchus, injuries to the left main bronchus are more often associated with pneumomediastinum and right main bronchus injuries are more commonly associated with pneumothorax.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


