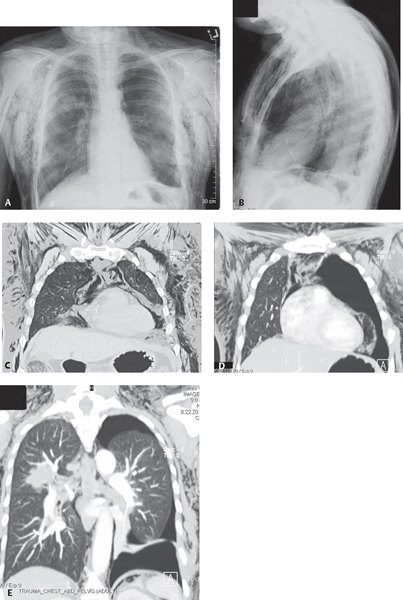
CASE 92 Middle-aged female victim of domestic violence brought into the Emergency Department after being severely beaten PA (Fig. 92.1A) and lateral (Fig. 92.1B) chest X-rays demonstrate extensive streaky lucencies of air in the mediastinum at the thoracic inlet and paralleling the superior vena cava and great vessels (Fig. 92.1A) and in the retrosternal clear space (Fig. 92.1B). A radiolucent line parallels the descending thoracic aorta from the aortic pulmonary window to the diaphragm (Fig. 92.1A). Extensive subcutaneous air is present in the chest wall and deep cervical fascia of the neck bilaterally. Right rib fractures are seen as well as an incidental right upper lobe mass (later diagnosed as primary lung adenocarcinoma). Coronal CT MIP (lung window) through the anterior (Fig. 92.1C), mid- (Fig. 92.1D), and posterior (Fig. 92.1E) thorax reveals extensive mediastinal air dissecting along the mediastinal pleural reflections of the heart and great vessels (Figs. 92.1C, 92.1D), descending aorta, and left diaphragm (Fig. 92.1E). A large left pneumothorax is seen, inconspicuous on the chest X-ray because of the extensive extra-alveolar air (Fig. 92.1E). Free air is present below the left diaphragm (Fig. 92.1E). The spiculated right upper lobe mass is also seen to better advantage (Fig. 92.1E). Pneumomediastinum None Pneumomediastinum is the presence of air or gas in the mediastinal compartment. It occurs in approximately 10% of blunt chest trauma victims but may also be seen with penetrating chest injuries. In more than 95% of cases, pneumomediastinum results from alveolar rupture following an abrupt increase in intra-alveolar pressure. The extra-alveolar air then dissects along the pulmonary interstitium and peribronchovascular sheaths centrally to enter the mediastinum (i.e., Macklin effect). Such abrupt increases in intra-alveolar pressure may occur with simple straining against a closed glottis (e.g., weight-lifting, childbirth), mechanical ventilation with barotrauma, or deep inhalation of illicit recreational drugs (e.g., crack cocaine, marijuana). Air may also enter the mediastinum from injuries to the aerodigestive tract (e.g., tracheobronchial tree, larynx, retropharynx, esophagus) or via the retroperitoneum. When extensive, air from the mediastinum can rupture into the pleural space, creating a pneumothorax; extend inferiorly into the retroperitoneum and rupture into the peritoneal space, resulting in pneumoperitoneum; or impede venous return to the heart (i.e., tension pneumomediastinum with cardiac tamponade).
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
92 Pneumomediastinum