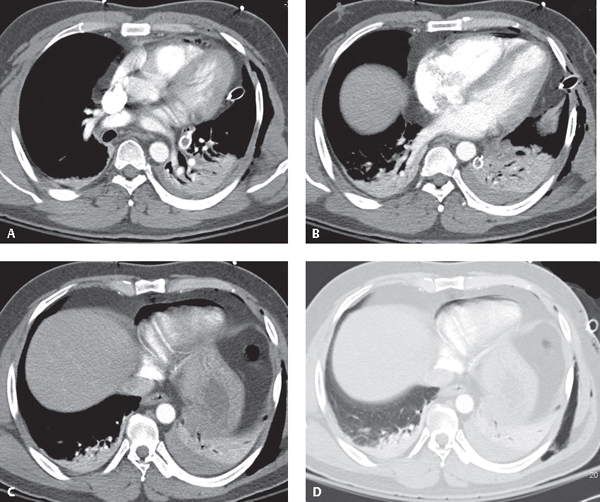
CASE 93 30-year-old man who sustained multiple stab wounds to his chest Contrast-enhanced chest CT (Figs. 93.1A, 93.1B, 93.1C, mediastinal window; Fig. 93.1D, lung window) demonstrates air in the pericardial sac and foci of pneumomediastinum. Note the concomitant left hemothorax, bibasilar volume loss, and subcutaneous air in the left chest wall. Pneumopericardium Fig. 93.1 None Pneumopericardium is defined as air within the pericardial sac. Post-traumatic pneumopericardium is rare; however, its presence is likely associated with an underlying cardiac injury. Pericardial and cardiac injuries are more commonly associated with penetrating as opposed to blunt trauma and result from direct violation of the pericardium and/or myocardium. Although less common with blunt thoracic trauma, injuries may occur following severe blows to the anterior chest. Such injuries may be complicated by cardiac contusion, cardiac rupture, valvular injuries, coronary artery injuries, conducting system injuries, hemopericardium, and cardiac tamponade. Pneumopericardium may result from cardiac or mediastinal surgery, penetrating or blunt trauma, infectious pericarditis with gas-producing organisms, and a fistulous communication between the pericardium and an adjacent air-containing organ (i.e., stomach or esophagus). Pneumopericardium secondary to blunt chest trauma is generally due to one of three mechanisms: (1) air extension along pulmonary venous perivascular sheaths from ruptured alveoli to the pericardium, (2) pneumothorax associated with pleuropericardial tear. or (3) direct tracheobronchial-pericardial communication. Cardiac contusion
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
![]()
Stay updated, free articles. Join our Telegram channel




Full access? Get Clinical Tree


