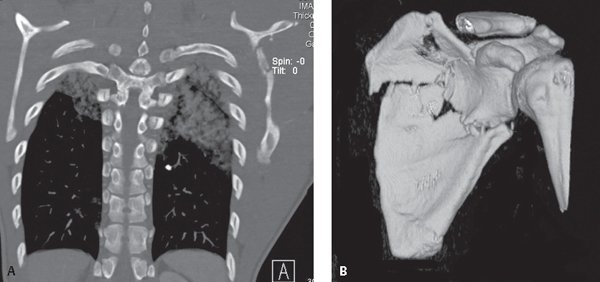
CASE 97 Young patient struck by a car Chest CT coronal MIP (bone window) (Fig. 97.1A) and 3-D reformatted image of the left scapula (bone window) (Fig. 97.1B) show a comminuted fracture of the scapula and bilateral upper lobe pulmonary contusions. 3-D reformation (Fig. 97.1B) reveals the articular surface of the glenoid is intact. Comminuted Left Scapular Fracture None Scapular fracture is present in approximately 1% of cases of blunt trauma. High-speed motor vehicle collisions are the most common cause of acute scapular fractures, but falls and direct blows to the area can also be responsible. A significant force is required to fracture the scapula. Therefore, the presence of such an injury should alert the radiologist and clinician to the possibility of additional thoracic injuries. Eighty to 90% of trauma patients with scapular fractures have associated rib fractures, pulmonary contusion (Fig. 97.1A), pneumothorax, or hemothorax. There is also a relationship between scapular fractures and thoracic spine as well as head injuries. Scapulothoracic dissociation is a rare but serious devastating closed forequarter amputation of the upper extremity resulting from a direct blow to or severe traction on the shoulder girdle. Fifty to 60% of patients with scapulothoracic dissociation are motorcyclists. The postulated mechanism of injury involves attempting to hold onto the handlebars while being forcibly thrown. Injuries to ATV riders occur in a similar manner and are becoming more common. Clinically, there is near complete disruption of the forequarter from the torso. Fig. 97.1 Signs and symptoms are similar to those of other acute fractures and include pain, tenderness, and reduced range of motion. Massive soft-tissue swelling and partial or complete tears of the deltoid, pectoralis minor, rhomboids, levator scapulae, trapezius, and latissimus dorsi muscles are usually present. Concomitant injury to the ipsilateral brachial plexus, subclavian artery, and/or subclavian vein invariably occurs. The axillary artery is not infrequently injured. The neurologic deficit is most often the result of complete avulsion of the brachial plexus. There is also a high prevalence of other, often severe injuries.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Clinical Findings
Scapular Fractures
Scapulothoracic Dissociation
Imaging Findings
Scapular Fractures
Chest Radiography
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


