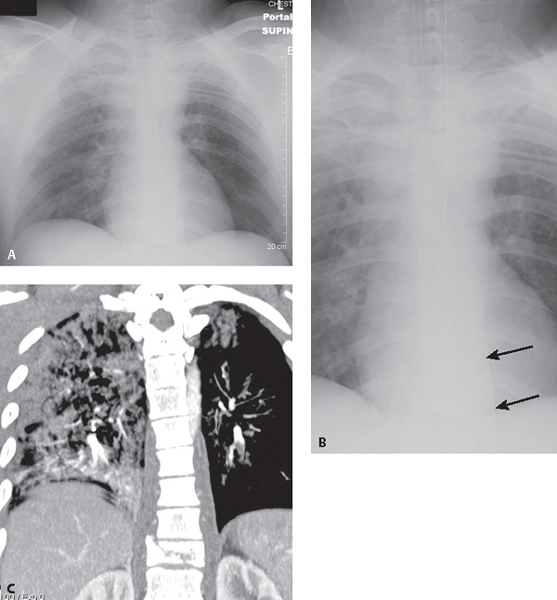
CASE 99 25-year-old man involved in a high-speed MVC with vehicular ejection AP chest radiograph (Fig. 99.1A) shows extensive right upper lobe and perihilar air space disease consistent with pulmonary contusions, and abnormal widening of the left, and to a lesser degree the right, paraspinal lines, which is seen to better advantage on the coned-down AP view (Fig. 99.1B) (arrows). Contrast-enhanced coronal MIP CT (Fig. 99.1C) demonstrates a burst fracture at T11. The associated paraspinal hematoma is responsible for the widened paraspinal lines seen on radiography. The multi-focal pulmonary contusions are also seen to better advantage. Fig. 99.1 Thoracic Spine Fracture with Paraspinal Hematoma • Other Causes of Post-Traumatic Mediastinal Hematoma (based on chest radiography) Thoracic spine fractures occur in 3% of blunt chest trauma victims. Compression fractures are the most common injury (52%) in the thoracic spine. Fracture-dislocation injuries of the thoracic spine account for 30% of all spine injuries. These latter injuries are often clinically devastating. The most vulnerable region of the spine is the functional thoraco-lumbar spine (i.e., T9–T11). However, over 20% of patients have multi-level injuries and the injuries may be non-contiguous in up to 27% of cases, factors radiologists must keep in mind during their interpretation of trauma chest CT scans. Seventy percent of acute thoracic spine fractures may be seen on radiography. However, the conspicuity of such fractures is dependent upon many factors, including radiologic technique, patient body habitus, concomitant pulmonary contusions and hemothorax, etc. As a result, many such fractures are not appreciated. Most injuries result from hyperflexion and axial loading.
 Clinical Presentation
Clinical Presentation
 Radiologic Findings
Radiologic Findings
 Diagnosis
Diagnosis
 Differential Diagnosis
Differential Diagnosis
 Discussion
Discussion
Background
Etiology
Clinical Findings
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


