Fig. 22.1
Layout of the MRXO. The surgical and angiography suite is in the middle, with MRI and CT suites located adjacent. The MRXO is also located next to the emergency medical unit
Concept of a Multimodal Imaging and Surgical Procedure Suite
This imaging and surgical suite is used for (1) combined use of various imaging modalities for interventional radiology, (2) intraoperative MRI and angiography, and (3) independent application of each imaging modality for diagnostic procedures if the modality is not in use for interventional procedure. The primary concept of the MRXO was focused on cost-effectiveness. In terms of cost-effectiveness, combining imaging equipment for interventional procedures is easy when only thinking about throughput. When imaging equipment is not in use for interventional procedures, routine diagnostic imaging can be performed. Routine imaging can thus be scheduled into the spaces between interventional procedures. Throughput of imaging equipment can thus be maximized.
On the other hand, use of intraoperative imaging is potentially problematic. Focusing on the throughput of the imaging system, if an MRI system is placed into the operation room, that system will only be used for surgery. The throughput of the system thus depends on the frequency of surgery. The question always arises about how often these interventional MRI scanners are used. On weekends, nights, and holidays, the MRI scanner in the operation suite is not available for use, while during the day on weekdays, the system is used once or, at most, twice a day. How do we best recoup the initial cost of introducing a high-field MRI scanner into the operation suite?
One solution to this problem is to reduce the initial cost of the scanner, such as by introducing a low-field imaging system [8, 9]. However, field strength affects both image quality and acquisition speed [10, 11]. In particular, low image quality greatly limits the interpretive ability of the radiologist. Alternatively, a mobile ceiling-mounted high-field MRI appears to represent one highly useful option for combined use of imaging equipment placed between a diagnostic imaging room and an operation room. The mobile MRI can be moved into the operation room when the surgeon needs intraoperative imaging, and this MRI can also be moved into the diagnostic imaging room for routine imaging. This is the main merit of this system: one MRI scanner uses both diagnostic imaging and intraoperative imaging.
Alternatively, patients can be moved between each modality. The University of California, San Francisco, opened a unique “twin bay” interventional suite coupling an angiography system with a 1.5 T MRI scanner [12]. The units, integrated into two rooms with an angiography system and MRI scanner placed exactly in-line, were connected with a movable tabletop that enables rapid transfer of the patient between the two rooms without changing position. A sliding door impenetrable to X-rays and radiofrequency power separates the two rooms. In order to maximize system usage, closure of the sliding door also allows the two modalities to be used independently for two patients simultaneously. This “twin bay” idea suggested an economical solution to the introduction of intraoperative MRI, as these suites can be used in combination for interventional procedures or independently for routine diagnostic procedures. This flexibility optimizes the throughput of each system and thus contributes to the cost-effectiveness.
Sharing Equipment Leads to Improved Cost-Effectiveness
The MRXO can be used totally independently, if all connecting doors are closed, even if routine imaging procedures are under way. We schedule three patients to undergo MRI, CT, and angiography simultaneously. During interventional radiology procedures, a radiologist performs manipulation of the catheter and monitors progress of the procedure. When a procedure calls for combined-modality imaging, the tabletop carrying the patient can be slid in a straight line through the open shielding door between the two rooms of the MRXO, showing reproducible imaging with minimal patient movement and time delay.
While routine surgical procedures are ongoing in the middle of the MRXO, the MRI and CT suites are available for patients who need routine diagnostic imaging. If the surgeon requires intraoperative images, the interventional patient can be inserted between routine diagnostic procedures. The MRI and CT scanners are then ready for additional routine diagnostic imaging. If routine diagnostic procedures are ongoing using MRI or CT, the surgical team must of course wait for the procedures to finish, but wait times are not overly long, and this delay is not a source of stress for the surgical team. The key concept behind the MRXO is “maximizing cost-effectiveness,” which led us to the system of sharing imaging modalities.
Use by Patients from the Emergency Room (ER) Increases Throughput
Another unique feature of the layout of this system is the placement of the MRXO next to the ER. The MRXO is conveniently available for emergency diagnostic imaging, if not in use for interventional radiology or surgical procedures. In particular, at night and on weekends and holidays, ER physicians are free to use the MRXO. Continuous use of the imaging modalities improves cost-effectiveness. In the first 5 years since the MRXO opened, the CT scanner has been used for routine imaging in an average of 35 cases a day, the MR scanner has been used for 16 cases a day, and diagnostic angiography has been used for 1 case a day [13]. This means that routine diagnostic procedures take up the free time in which the imaging systems are not in use for interventional procedures.
Layout of the MRXO
The MRXO has three imaging systems (MRI, CT, and angiography) and one fully functional operation room, with these four functions condensed into three rooms. In the middle of the suite is the combined operating suite and angiography suite, while the MRI suite and CT suite are each installed in an adjoining bay connected to the surgical and angiography suite. Each adjoining bay is connected by specially designed radiofrequency, X-ray, and magnetic-shielded sliding doors. The tables for MRI, angiography, CT, and surgery are placed in a perfectly straight line, with the movable tabletop carrying the patient sliding along this line (Fig. 22.2).
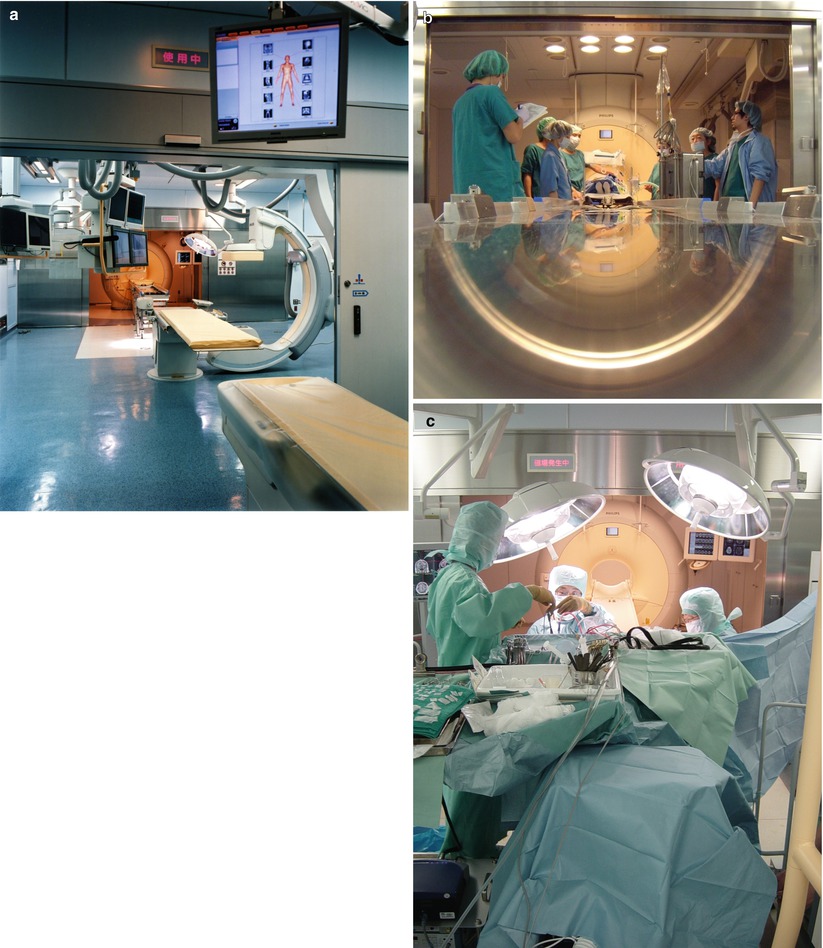
Fig. 22.2
(a) Layout of the MRXO. View from the CT suite into the MRI suite through the surgical and angiography suite. Note that the MRI, angiography, and CT suites are exactly in-line. (b) View over the operating table base. The operating table is in a perfectly straight line with the MRI scanner. (c) View over the operating field to the MRI suite. The mobile nurse platform carrying all ferromagnetic surgical instruments (e.g., motor for high-speed drills, suction systems, electrocoagulator, bipolar coagulator system) protrudes over the operating table
The surgical and angiography suite placed in the middle is the key functional room in the MRXO. This surgical and angiography suite can be used for neurosurgical procedures and is fitted with surgical lights, a laminar air flow ventilation system with microbiological filter, electrical outlets, medical gas supplies, patient monitors, and a surgical navigation system. Preparation for interventional radiology is performed in the surgical and angiography suite. After catheter manipulation and surgical procedures in this suite, the patient is moved to the MRI or CT suite for imaging. Electrical outlets and medical gas supplies for anesthesia are also installed in both CT and MRI suites. Clean air ventilation with a microbiological filter system and MRI-compatible surgical lights is installed in the MRI suite to maintain cleanliness and brightness.
What Is the Increase in Initial Cost?
Of course, some modification of the docking system is needed to connect each imaging system to the others and to the operating table. In general, in terms of initial cost, modifying the imaging equipment increases the price by about 15 %. One factor affecting the cost-effectiveness of the MRXO suite is the ease and frequency with which the shared imaging equipment can be used for routine surgery, diagnostic procedures, and treatments.
Specially Designed Operation Table and Connection Bridge
In neurosurgical operations under microscopy that require changes in position of the patient’s head (i.e., elevation, descent, rotation right and left), light direction of the microscope must frequently be followed. Currently, MRI-compatible operation tables generally have an inflexible, flat, tight tabletop. Using such tabletops is often difficult for neurosurgeons, as cerebrospinal fluid and venous drainage are insufficient during the surgery, and positioning of the microscope in the tight surgical field is difficult. We use a fully functional flexible operating table (MST-7201-BX; Mizuho Ikakogyo, Tokyo, Japan) carrying a special MRI-compatible tabletop (Fig. 22.3) [7]. The flexible MRI-compatible operating table provides the same range as routine neurosurgical operation tables currently used by neurosurgeons in specialized operation rooms. The table base carries a special MRI-compatible tabletop that is divided into three parts (Fig. 22.4a). When the surgeon requires intraoperative MRI, the tabletop must be placed in a flat position and a spacer inserted into each of the tabletop joints (Fig. 22.4b). The spacers tightly lock the three parts of the MRI-compatible tabletop together. At this point, the flexible MRI-compatible tabletop is flat and quite inflexible. The MRI-compatible tabletop is then released from the table base, and the patient easily slides on the MRI-compatible tabletop from the operation and angiography suite into the MRI suite.
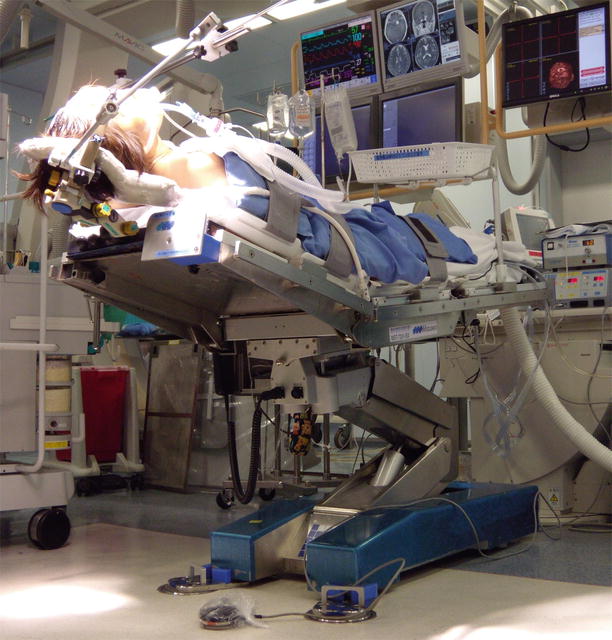
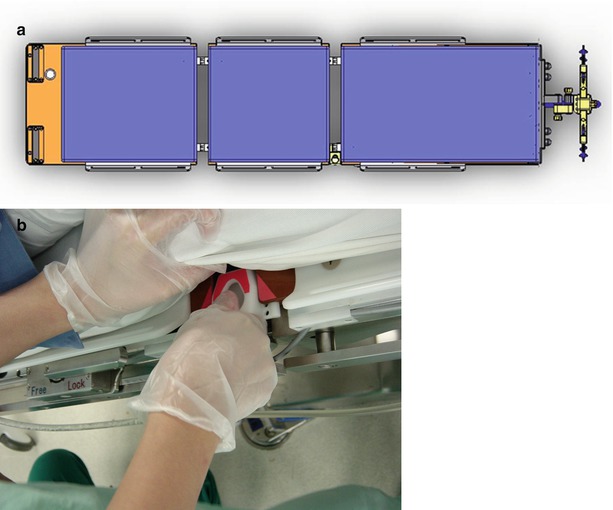
Fig. 22.3
The fully functional flexible operating table is mounted on a special MRI-compatible tabletop to carry the patient. The operating table allows the surgeon to control Trendelenburg or reverse Trendelenburg position, body rotation toward to the right or left, foot elevation, and head elevation, with a minimum height of 480 mm and a maximum height of 1,100 mm
Fig. 22.4
(a) The special MRI-compatible tabletop, which is divided into three parts. (b) When the surgeon wishes to perform MRI, the tabletop is placed in a flat position and a spacer inserted into each of the two tabletop joints. The spacers tightly lock the three parts of the tabletop together
Steps for Intraoperative MRI
Intraoperative imaging can be performed at any time, provided that the usual precautions are taken to ensure sterility. All ferromagnetic instruments are removed from the surgical field, and the surgical wound is covered with a sterile drape. No infectious complications related to neurosurgical procedures have been encountered since the opening of the MRXO. During preparation for imaging, the craniotomy area is temporarily covered with a sterile drape. After imaging, this sterile drape is removed from the patient’s head, and a new drape is applied to the craniotomy area. Using this draping technique, sterility of the craniotomy area is maintained. The connecting bridge is placed between the MRI-compatible tabletop-mounted operating table and the MRI table (Fig. 22.5a). The patient can be moved in and out of the MRI scanner in about 10–20 s. The results of imaging may determine the surgical approach by revealing the presence of residual tumor that can be safely removed. After intraoperative imaging, the patient is returned to the primary surgical position, and resection is continued (Fig. 22.5b).

 Visualization and Display for Image-Guided Therapy
Visualization and Display for Image-Guided Therapy
 Multimodality Navigation in Neurosurgery
Multimodality Navigation in Neurosurgery
 Image-Guided Robotics in Minimally Invasive Therapies
Image-Guided Robotics in Minimally Invasive Therapies
 Innovations in Ultrasound Instrumentation for Image Guidance
Innovations in Ultrasound Instrumentation for Image Guidance
 Image-Guided Prostate Brachytherapy
Image-Guided Prostate Brachytherapy
 CT-Guided Interventions: Current Practice and Future Directions
CT-Guided Interventions: Current Practice and Future Directions




Related posts:
Visualization and Display for Image-Guided Therapy
Multimodality Navigation in Neurosurgery
Image-Guided Robotics in Minimally Invasive Therapies
Innovations in Ultrasound Instrumentation for Image Guidance
Image-Guided Prostate Brachytherapy
CT-Guided Interventions: Current Practice and Future Directions
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
