Imaging is essential in management of suspected abdominal masses. Data to be obtained are the composition of the mass (solid, cystic, or mixed), its limits, its location and organ dependence, its vascularization, and the presence of additional findings (lymphadenopathy, ascites, etc.). Afterward, an approximation about the nature of the mass (benign/malignant) and a possible differential diagnosis can be inferred. US is almost always the first imaging modality used, and can provide essential information. CT, MR, NM, and PET are useful to complete the diagnosis.
Table 2.64 Neonatal cystic masses
Diagnosis
Findings
Comments
Hydronephrosis
Depending if uni-/bilateral and on level of obstruction.
Most common mass in neonate. Usually diagnosed in utero.
Multicystic dysplastic kidney
Cluster of cysts in renal fossa In rare occasions may be focal.
Multilocular, thin wall, grows among other structures without displacing.
Sacrococcygeal teratoma
Mixed cystic-solid pattern.
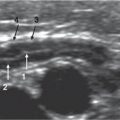
Fig. 2.135a, b Hydrometrocolpos. A newborn with abdominal distension. (a) Plain film depicts a pelvic mass with intestinal loop displacement. (b) Sagittal pelvic US obtained after partial drainage shows a fluid-filled vagina and a uterus with mildly distended endometrial lumen, located behind the bladder.Fig. 2.136 Peritoneal lymphangioma. Transverse US image in mesogastrium depicts a characteristic polylobulated cystic mass with thin septa.
Table 2.65 Neonatal solid masses
Diagnosis
Findings
Comments
Polycystic kidney disease
Bilateral enlarged distorted kidneys.
In autosomal recessive form.
Mesoblastic nephroma
Large ill-defined mass.
May be cystic.
Renal ectopia
Empty renal fossa.
Usually pelvic kidney or crossed-fused ectopia.
Renal vein thrombosis
Unilateral enlarged kidney with absent flow (acute phase), subsequent atrophy.
Secondary to dehydration, sepsis, umbilical vein catheterization.
Nephroblastomatosis-Wilms tumor
Large tumors unior multifocal and unior bilateral.
Most common solid renal mass in children.
Neuroblastoma
Large, heterogeneous, irregular mass. Adrenal, retroperitoneum, or other locations.
Fig. 2.137a, b Mature teratoma in a 13-year-old girl. Sagittal (a) and transverse (b) US images show a complex cystic mass cranial to the uterus and positioned over the bladder with solid hyperechoic components representing fat and hairs, which was confirmed at pathologic examination.
Table 2.67 Older children solid masses
Diagnosis
Findings
Comments
Wilms tumor
Large tumor, hypervascular, heterogeneous. May invade IVC and cross midline.