principle are vitally important for the pediatric angiographer. Angiography, particularly during lengthy percutaneous interventions, has the potential to deliver the highest radiation dose of any imaging study. Methods to reduce radiation exposure during fluoroscopy include the use of pulse fluoroscopy, last-image hold, copper filtration, optimal collimating, and removal of anti-scatter grids while imaging neonates and small infants.
 FIGURE 20.1 Diagram of peritoneal spaces. |
the peritoneal ligaments are the greater sac and the lesser sac, also known as the omental bursa.
 FIGURE 20.2 A 13-year-old girl on peritoneal dialysis undergoing CT peritoneogram to assess for peritoneal adhesions. Contrast opacification of the peritoneum identifies the major spaces and ligaments. RSP, right subphrenic space; LSP, left subphrenic space; GHL, gastrohepatic ligament; HDL, hepatoduodenal ligament; LS, lesser sac; S, stomach; P, pancreas; D, duodenum; RPC, right paracolic space; LPC, left paracolic space; PS, pelvic space. (Image courtesy of Jonathan R. Dillman, MD, MSc, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH.) |
TABLE 20.1 Anatomic Spaces of the Peritoneal Cavity | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
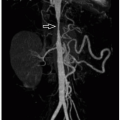
 FIGURE 20.3 Normal angiographic anatomy of the abdominal aorta and its visceral branches. Arrows indicate the major abdominal aortic visceral branches. CHA, common hepatic artery; SA, splenic artery; RRA, right renal artery; LRA, left renal artery; SMA, superior mesenteric artery. |
 FIGURE 20.4 Normal inferior vena cavogram. The ostia of the renal veins are identified as jets of unopacified blood (arrows) flowing into the inferior vena cava. |
 FIGURE 20.5 Normal angiographic anatomy of the superior mesenteric artery (SMA) and its branches. On the right, the inferior pancreaticoduodenal artery (IPDA) anastomoses with the superior pancreaticoduodenal artery branch of the gastroduodenal artery, forming a collateral pathway between the SMA and celiac axis. There are multiple left-sided jejunal branches (JB). On the right are the middle colic (MCA), right colic (RCA), and ileocolic arteries (ICA), and anastomoses among these arteries form a marginal artery (of Drummond) that irrigates the right and transverse colon. Distal to the origin of the ICA, multiple ileal branches (IB) supply the ileum. |
TABLE 20.2 Collateral Pathways of Mesenteric Arteries | ||||||||
|---|---|---|---|---|---|---|---|---|
| ||||||||
This artery is the smallest of the mesenteric arteries and nourishes the distal transverse colon, descending colon, sigmoid colon, and rectum. The major branches of the IMA are the left colic, sigmoid, and hemorrhoidal arteries, all of which branch off to the left. The left colic ascends from its origin off the IMA to anastomoses with branches from the SMA. In ˜12% of individuals, the left colic artery is absent. In this situation, the perfusion of the descending and sigmoid colon is provided by the colosigmoid artery. Occasionally, the left colic artery may arise from the SMA. The left colic artery extends cephalad to the splenic flexure in the majority of patients and reaches the mid-aspect of the transverse colon in ˜15% to 20% of patients. However, perfusion of the splenic flexure is highly variable, and in some patients, the middle colic artery may be the only artery irrigating this territory.
 FIGURE 20.6 Normal angiographic anatomy of the inferior mesenteric artery (IMA). The left colic artery (LCA) anastomoses with the middle colic artery of the superior mesenteric artery (SMA) to provide SMA-IMA collaterals. Multiple sigmoid branches (SB) arise from the IMA, and the terminal branch of which is the superior hemorrhoidal artery (SHA). |
 FIGURE 20.7 Superior mesenteric vein (SMV) appearance on CT. Maximum intensity projection reconstruction CT image demonstrates the normal anatomy of the SMV. This vein receives blood from multiple mesenteric veins, which coalesce most commonly into a single trunk that subsequently joins with the splenic vein to form the portal vein (PV). |
Typically an omphalocele is diagnosed on prenatal US showing an anterior midline herniation with a covering membrane (Fig. 20.8) and the umbilical cord vessels seen inserting at the base of the hernia.
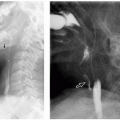
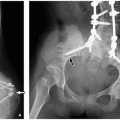
 FIGURE 20.8 Imaging features of omphalocele and gastroschisis. A: Abdominal radiograph of a neonatal boy with omphalocele demonstrates a large anterior abdominal wall hernia (arrow) containing the stomach (asterisk) and multiple bowel loops. B: Prenatal sagittal T2-weighted MRI of a fetal omphalocele at 32 weeks of gestational age demonstrates an anterior abdominal hernia containing the liver covered by a thin outer membrane (asterisk), with the umbilical cord vessels inserting at the hernia base (arrow). In contrast, prenatal imaging of a 25-week-gestational-age fetus with gastroschisis on ultrasound (C) and sagittal T2-weighted MR image (D) demonstrate anterior herniation of small bowel loops (arrowheads) with no outer covering membrane. (Radiograph [A] provided by Jonathan R. Dillman, MD, MSc, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH. Ultrasound [C] and MRI [B and D] images provided by Sudha Anupindi, MD, and Teresa Victoria, MD, Children’s Hospital of Philadelphia, Philadelphia, PA.) |
mesodermal development, leading to urinary tract distention, abnormal abdominal wall muscular development, and failure of testicular descent.16,17 The abdominal wall defect classically consists of disorganized central abdominal wall muscles that are infiltrated with collagen bundles.18 Cryptorchidism has been attributed to both impeded testicular descent by the distended urinary system as well as atresia of the gubernaculum, which does not pull adequately.16
 FIGURE 20.9 Prune belly syndrome in a newborn boy. A: Radiograph demonstrates marked abdominal wall laxity. B and C: Renal ultrasound images show bilateral hydronephrosis. The kidneys are echogenic and contain several small cysts, suggestive of underlying renal dysplasia. |
be accompanied by fever or malaise. Most commonly, cellulitis is a complication of an overlying skin disorder, such as a penetrating wound (including a puncture, abrasion, or bite), ulcer (e.g., varicella lesions or newborn omphalitis), or dermatosis.27,28 Abdominal wall cellulitis in children may also be a sequela of abdominal surgery, such as appendectomy. Most cases of cellulitis are due to infection by Streptococcus and Staphylococcus skin flora. Less typical organisms include oral flora in cases of cellulitis secondary to a bite or Gram-negative rods, anaerobic flora, and fungi in immunocompromised patients.28
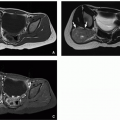
 FIGURE 20.10 Proteus syndrome in an 15-year-old boy. Axial enhanced CT images demonstrate a vascular malformation (A; arrows) in the right flank abdominal wall as well as a large abdominal wall lipoma (B; asterisk). |
 FIGURE 20.11 Abdominal wall cellulitis in a newborn boy. A: Gray-scale ultrasound image of the paraumbilical region demonstrates heterogeneous thickening of the paraumbilical abdominal wall soft tissues, consistent with cellulitis. B: Color Doppler ultrasound image shows mild hyperemia. |
(<5 per million annual incidence) arise mostly in young adults and less commonly in children, with a slight female predominance and peak incidence in the third and fourth decades.31 Desmoid tumor locations are traditionally classified as intraabdominal (mesenteric or pelvic), abdominal wall, or extra-abdominal (most commonly in the proximal extremities, head, and neck). Patients with Gardner-type familial adenomatous polyposis (FAP) have a >800-fold increased incidence of desmoids, which are usually intra-abdominal or mesenteric in location.32,33 Abdominal wall desmoids occurring in the rectus abdominis or internal oblique muscles have an association with pregnancy.34 Desmoid tumors usually occur as single tumors, although ˜15% are multiple.34
 FIGURE 20.12 Abdominal wall desmoid tumor in a 17-year-old boy with Gardner syndrome. Sagittal T2-weighted (A) and postcontrast T1-weighted fat-saturated (B) MR images demonstrate a hyperintense and enhancing mass (arrows) centered in the rectus abdominis muscle, consistent with known desmoid tumor. |
In children, soft tissue sarcomas occurring in the abdominal wall are primarily nonrhabdomyosarcoma soft tissue sarcomas (NRSTS). Such NRSTS are a heterogeneous group of histologic subtypes derived from mesenchymal cells, which often have characteristic genetic translocations that aid in their diagnosis.40 This includes infantile fibrosarcoma, which is a rare NRSTS that occurs specifically in infants under 2 years of age (median age 3 months) and presents typically as a large infiltrative soft tissue mass with associated skin discoloration that may mimic vascular malformation.42 Synovial sarcoma (Fig. 20.14) is one of the common sarcomas in older children. All NRSTS typically present as a slowing growing and painless mass.
 FIGURE 20.13 Gross appearance of desmoid fibromatosis developing after ileostomy closure in an 18-year-old man with familial adenomatous polyposis. The 5 cm mass ( asterisk) is firm and pale tan, distinct from the red-brown abdominal musculature. |
 FIGURE 20.14 Gross appearance of a synovial sarcoma from the abdominal wall of a 13-year-old boy. This is a 6.5 cm tumor resected after chemotherapy. The tumor (asterisk) is multilobular and light tan with soft pale areas of necrosis. |
 FIGURE 20.15 Abdominal soft tissue sarcoma in a 17-year-old boy. A: Sagittal enhanced CT image demonstrates a soft tissue mass (arrow) in the abdominal wall. B: Ultrasound depicts the lesion as a hypoechoic mass (calipers) with internal Doppler vascularity. C: Ultrasound-guided percutaneous core needle biopsy of the lesion established the diagnosis of synovial sarcoma. |
primarily as a result of high-energy lap-belt trauma during motor vehicle collisions or from low-energy falls onto bicycle handlebars (the so-called handlebar hernia).49,50,51 The vast majority of these injuries that are bicycle related are in boys, with a mean age of ˜10 years.51
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


