Abnormalities of the Saphenous Nerve at the Ankle
Anatomic Considerations
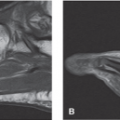
The saphenous nerve is the largest sensory branch of the femoral nerve. The saphenous nerve provides sensory innervation to the medial malleolus, the medial calf, and a portion of the medial arch of the foot. The saphenous nerve is derived primarily from the fibers of the L3 and L4 nerve roots. The nerve travels along with the femoral artery through Hunter’s canal and moves superficially as it approaches the ankle (Fig. 11.1). It passes over the medial malleolus of the tibia, splitting into terminal sensory branches (Figs. 11.2 and 11.3). The saphenous nerve is subject to trauma or compression anywhere along its course. The nerve is frequently traumatized during vein harvest for coronary artery bypass grafting procedures. The saphenous nerve is also subject to compression as it passes over the medial condyle of the femur. Less commonly, the nerve is damaged or compressed distally as it passes beneath the fascia of the dorsum of the foot.
Clinical Correlates
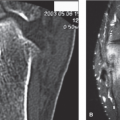
Saphenous neuralgia is caused by entrapment and compression of the saphenous nerve anywhere along its course, with compromise of the nerve most common as it passes through Hunter’s canal, at the medial condyle of the femur, and as it passes beneath the fascia of the dorsum of the foot (Fig. 11.1). The saphenous nerve is frequently traumatized during vein stripping and harvest procedures, with the infrapatellar branch of the saphenous nerve frequently damaged during total knee arthroplasty (Fig. 11.4). The nerve can also be damaged by trauma to the ankle, including fracture, dislocation, and crush injuries (Figs. 11.5 and 11.6). The musculotendinous units of the tibialis muscles are subject to the development of tenosynovitis which may also compromise the nerve.
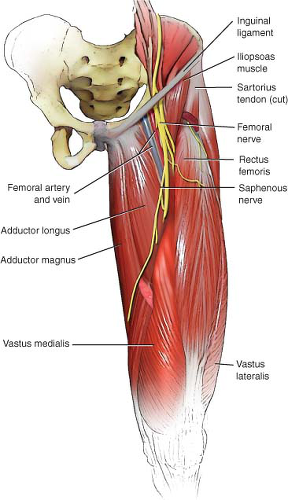 FIGURE 11.1 The anatomy of the proximal saphenous nerve. |
Electrodiagnostic testing should be considered in all patients who suffer from saphenous nerve dysfunction to provide both neuroanatomic and neurophysiologic information regarding nerve function. Magnetic resonance imaging and ultrasound imaging of the popliteal fossa as well as anywhere along the course of the saphenous nerve are also useful in determining the cause of saphenous nerve compromise.
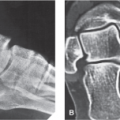
Plain radiographs of the ankle should be obtained in all patients who have trauma to the ankle, to rule out fractures of the medial ankle which can damage the saphenous nerve (Fig. 11.7).
Plain radiographs of the ankle should be obtained in all patients who have trauma to the ankle, to rule out fractures of the medial ankle which can damage the saphenous nerve (Fig. 11.7).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


