Abnormalities of the Talofibular Ligament
Anatomic Considerations
The ankle is a hinge-type articulation between the distal tibia, the two malleoli, and the talus (Fig. 4.1). The articular surface is covered with hyaline cartilage, which is susceptible to arthritis. The joint is surrounded by a dense capsule that helps strengthen the ankle. The joint capsule is lined with a synovial membrane that attaches to the articular cartilage. The ankle joint is innervated by the deep peroneal and tibial nerves.
The major ligaments of the ankle joint include the talofibular, anterior talofibular, calcaneofibular, and posterior talofibular ligaments, which provide the majority of strength to the ankle joint (Fig. 4.2). The talofibular ligament is not as strong as the deltoid ligament and is susceptible to strain. The talofibular ligament runs from the anterior border of the lateral malleolus to the lateral surface of the talus (Fig. 4.3).
 FIGURE 4.1 The articulations of the ankle joint. |
Clinical Correlates
One of the four major ligaments of the ankle joint, the anterior talofibular ligament runs from anterior border of the lateral malleolus to the lateral surface of the talus (Fig. 4.3). Also known as the medial ligament of talocrural joint, the anterior talofibular ligament is susceptible to strain at the joint line or avulsion at its origin or insertion. The anterior talofibular ligament is frequently injured from inversion injuries to the ankle that occur when tripping when wearing high heels, landing hard or running on hard uneven surfaces, and during dancing, soccer, and basketball (Fig. 4.4). The pain of anterior talofibular ligament damage is localized to the lateral ankle and is made worse with inversion of the ankle joint. Point tenderness just below the lateral malleolus is often present on physical examination. Significant swelling and ecchymosis are often evident
after acute injury. Activity, especially involving weight bearing, plantar flexion, and inversion of the ankle will exacerbate the pain. Local heat and decreased activity as well as elevation of the affected ankle may provide a modicum of relief. Sleep disturbance is common in patients suffering from trauma to the anterior talofibular ligament of the ankle. Coexistent fracture, bursitis, tendinitis, arthritis, or internal derangement of the ankle may confuse the clinical picture after trauma to the knee joint making clinical diagnosis difficult (Fig. 4.5).
after acute injury. Activity, especially involving weight bearing, plantar flexion, and inversion of the ankle will exacerbate the pain. Local heat and decreased activity as well as elevation of the affected ankle may provide a modicum of relief. Sleep disturbance is common in patients suffering from trauma to the anterior talofibular ligament of the ankle. Coexistent fracture, bursitis, tendinitis, arthritis, or internal derangement of the ankle may confuse the clinical picture after trauma to the knee joint making clinical diagnosis difficult (Fig. 4.5).
 FIGURE 4.2 The major ligaments of the ankle joint include the talofibular, anterior talofibular, calcaneofibular, and posterior talofibular ligaments, which provide the majority of strength to the ankle joint. (From Patel A, Horton G. Anatomy of the foot and ankle. In: Altcheck DW, DiGiovanni CW, Dines JS, et al, eds. Foot and Ankle Sports Medicine. Philadelphia, PA: Lippincott Williams & Wilkins; 2013:2.) |
 FIGURE 4.3 Anatomy of the anterior talofibular ligament and its relationship with the other ligaments of the lateral ankle. (Anatomical Chart Company, 2013.) |
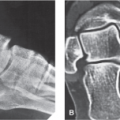
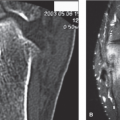
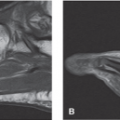
Plain radiographs and/or arthrography are indicated in all patients who present with anterior talofibular ligament pain, especially after ankle trauma (Fig. 4.6). Based on the patient’s clinical presentation, additional testing may be indicated, including complete blood cell count, sedimentation rate, and antinuclear antibody testing. MRI or ultrasound imaging of the ankle is indicated if internal derangement or occult mass or tumor is suspected as well as to confirm the diagnosis of suspected anterior talofibular ligament injury (Figs. 4.7 and 4.8). Bone scan may be useful to identify occult stress fractures involving the joint, especially if trauma has occurred.
Ultrasound Technique
To perform ultrasound evaluation of the talofibular ligament, the patient is placed in the lateral curled up position with the affected ankle facing up. A high-frequency linear ultrasound transducer is then placed in the transverse position with the posterior aspect of the transducer placed just over the bottom of the lateral malleolus (Fig. 4.9). A survey scan is taken which demonstrates the hyperechoic anterior talofibular ligament running from the talus to the lateral malleolus of the fibula (Fig. 4.10). After the anterior talofibular ligament is identified, the ligament is evaluated for edema, strain, tears, and rupture (Figs. 4.11 to 4.21). A careful search for avulsion fractures at the insertions of the anterior talofibular ligaments should then be carried out (Fig. 4.22). Color Doppler may aid in the assessment of the extent of acute ligament injury (Fig. 4.23).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


