Acetabulum
Anthony J. Wilson
John H. Harris Jr.
Fractures of the acetabulum are generally considered to be different than other pelvis fractures because they involve the hip joint, the largest weight-bearing joint in the body. Unlike pelvic ring injuries, isolated acetabular fractures are not usually life threatening. However, they can have significant long-term sequelae. These sequelae can be minimized by anatomic reduction and stabilization. For many years, orthopedic surgeons have used the classification system of Letournel and Judet for acetabular fracture evaluation and surgical planning. Because surgical approaches and fixation methods vary with the classification, accurate classification of these fractures is important for worthwhile communication between radiologist and orthopedist.
Traditionally, the mainstay of classification has been pelvic radiographs. The standard workup has consisted of three projections: an anteroposterior (AP) view and two oblique views, with all three covering the entire pelvis. Orthopedists usually refer to the oblique views as “Judet views.” The anterior and posterior oblique projections of each hip demonstrated on the Judet views are known as the “ obturator” and “iliac” obliques, respectively. In more recent years, computed tomography (CT) has also become a popular method for preoperative planning. There have been differences of opinion between different observers concerning the need for multiplanar and 3-D reformations and their value. Some observers have suggested that multiplanar reformations of CT should replace the radiographs and recent studies have supported this concept. A clear understanding of both the standard radiographs and axial and reformatted CT images is important in accurately classifying acetabular fractures.
THE COLUMN PRINCIPLE
In his 1993 book, Letournel described the acetabular column principle. This principle considers the hemipelvis to be an inverted “Y” with a “C” shaped acetabular articular surface positioned between the limbs of the “Y” (Fig. 18.1). The transmission of weight-bearing loads from the lower extremity to the spine is via the anterior and posterior limbs of the “Y,” known as the anterior and posterior columns, respectively. Immediately adjacent to these columns are the anterior and posterior walls of the acetabulum. The classification system of Letournel and Judet simply analyzes the patterns of involvement of the columns and walls.
RADIOGRAPHIC EVALUATION
On the AP radiograph, cortical lines can be found, which are markers for the columns and walls (Figs. 18.2 and 18.3). The marker for the anterior column is an anterior cortical line, extending from ilium to pubis, known as the iliopectineal line. The marker for the posterior column is a posterior cortical line extending from ilium to ischium, known as the ilioischial line (Fig. 18.2). Two oblique cortical lines can usually be found projecting through the femoral head. The more lateral and slightly more vertical of these lines is the edge of the posterior acetabular wall. The more medial and slightly more horizontal line is the edge of the anterior wall (Fig. 18.3). The posterior wall should always be visible on a good quality AP radiograph, but the anterior wall is not always so well defined.
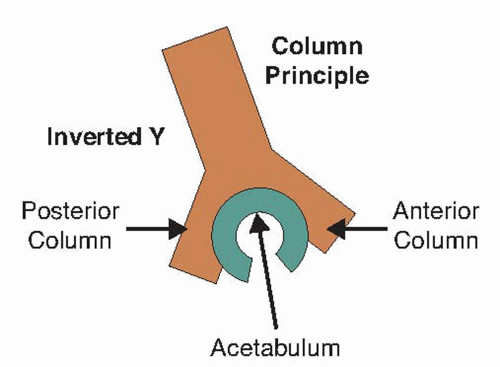 Figure 18.1. The column principle of Letournel and Judet. |
COMPUTED TOMOGRAPHIC EVALUATION
It is essential to carefully evaluate each axial CT slice for subtle injuries. However, the most helpful axial CT image for classifying acetabular fractures is the one that passes through the roof or “tectum” of the acetabulum (Fig. 18.4). The orientation of the fracture on this image is the most important clue to the correct classification and extensions of the fracture into the iliac wing; posterior column, anterior column, and/or obturator ring will give further clues to the correct classification.
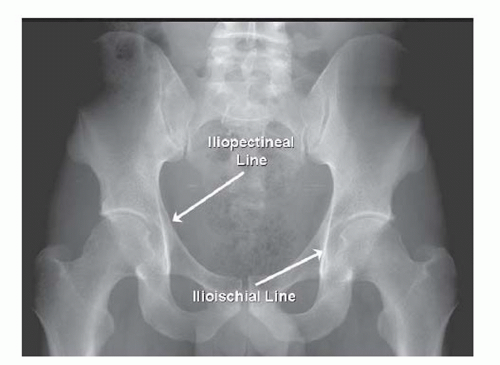 Figure 18.2. The radiographic markers for the anterior and posterior columns. |
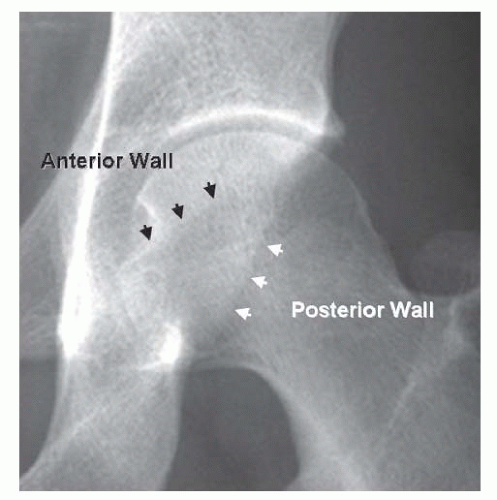 Figure 18.3. The location on an anteroposterior radiograph of the anterior and posterior walls of the acetabulum. |
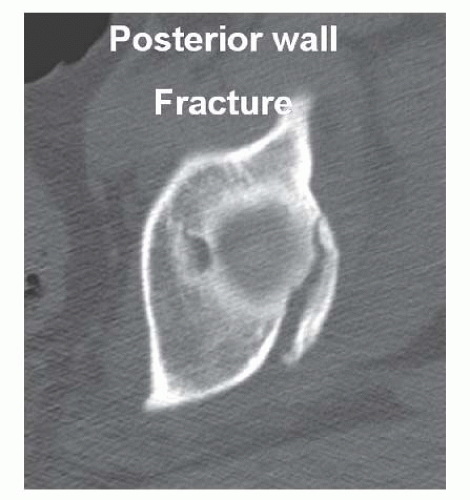 Figure 18.4. Axial CT scan through the acetabular tectum, showing the oblique orientation of a posterior wall fracture. |
CLASSIFICATION
Letournel and Judet described five basic or “elemental” patterns of acetabular fractures and five combined patterns. Four of the basic fracture patterns divide the acetabulum into anterior and posterior sections. Each of these four elemental fractures involves only a single column or wall. A fifth elemental fracture divides the acetabulum transversely into superior and inferior components and extends across both of the columns. Thus, the five elemental patterns are anterior column, posterior column, anterior wall, posterior wall, and transverse (Fig. 18.5). All of the combined patterns include two or more of these elements. The five combined patterns are posterior column with posterior wall, both columns, transverse with posterior wall, transverse with “T” extension, and anterior column with posterior hemitransverse (Fig. 18.6).
Although at first this classification sounds complicated and difficult to remember, it can be simplified by listing the different fracture types into three categories: column fractures, wall fractures, and transverse fractures (Fig. 18.7). Most of the combined patterns fall into more than one of these categories. An additional factor that helps with sorting out the patterns is the fact that some of the patterns are distinctly uncommon. Studies have shown that posterior wall fractures, both-column fracture, and transverse fracture variants account for well more than 90% of all acetabular fractures. Thus, if the observer can separate these three patterns, classification of most acetabular fractures becomes easy.
Separating these three fracture patterns is not difficult as long as the observer follows a few simple principles. Isolated posterior wall fractures are unlikely to be confused with the other two common patterns because of the posterior wall fracture’s simplicity, different location, and different orientation. The problem then becomes how do you separate both-column pattern from the transverse varieties, as all of these fractures involve both of the acetabular columns? The distinction between these two is also straightforward. All column fractures divide the acetabulum vertically into anterior and posterior components and appear as coronal fractures of an axial CT image of the acetabular tectum (Fig. 18.8). All transverse fractures divide the acetabulum horizontally into superior and inferior components and appear as sagittal fractures on an axial CT image of the acetabular tectum (Fig. 18.9). Additionally, both-column fracture start in the iliac wing and extend inferiorly through the iliopectineal line, ilioischial line, and ischiopubic ramus. All transverse fractures also extend through both the iliopectineal and ilioischial lines, and although the T-shaped variant includes an ischiopubic ramus fracture, there is no transverse pattern that extends upward into the iliac wing.
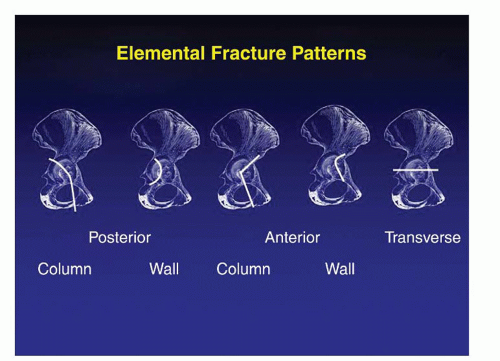 Figure 18.5. The five elemental fracture patterns of Letournel and Judet. |
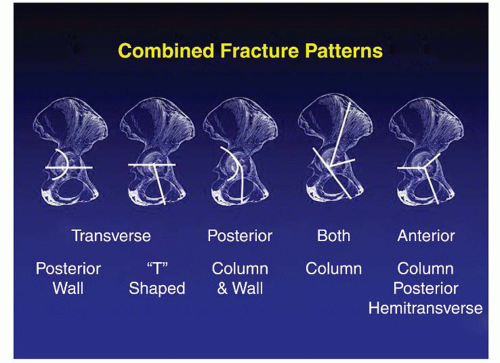 Figure 18.6. The five combined fracture patterns of Letournel and Judet. |
On the initial evaluation, the observer should determine if the iliopectineal line, the ilioischial line, or both lines are disrupted. If both are disrupted, the choice lies between a transverse variant and both-column fracture (Figs. 18.10 and 18.11). If the fracture extends up into the ilium, both-column fracture is most likely. However, the final proof can be obtained from the orientation of the fracture on an axial CT image of the acetabular tectum (Figs. 18.4, 18.8, 18.9, and 18.12).
Acetabular wall fractures, whether isolated or combined, will appear as oblique fracture lines on the tectal CT image (Fig. 18.4). Posterior wall fractures, although usually visible and diagnosable on AP radiographs, are more clearly demonstrated by an obturator oblique view (Fig. 18.13).
Combined fracture patterns such as transverse/posterior wall or anterior column/posterior hemitransverse will show combinations of the earlier fracture orientations on the tectal CT image.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


