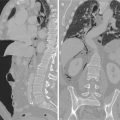
Fig. 7.1
MDCT MPR coronal oblique image shows inflammation of the appendix with fluid-filled lumen, associated to inflammatory thickening of the caecal wall
In cases of severe appendicitis, it is important to identify the presence of potential complications and mainly perforation. Presence of perforation significantly increases morbidity and mortality [3] and can condition therapeutic treatment. In some cases when it is present, often associated to abscess formation, surgical treatment is avoided in a first-line choice and medical therapy or percutaneous drainage is preferred. Perforation dramatically increases the risk of complications after surgical period.
From this aspect comes the importance of a correct pathology definition in the preoperative setting using a high sensitive and specific technique.
There are five MDCT signs of appendix perforation which are very specific:
Get Clinical Tree app for offline access

Enhancing defect foci of the wall: it has high sensitivity, specificity and accuracy (95, 97 and 96 %, respectively) [3]. Some authors, otherwise, underline the possibility of artefact presence that hampers the utility of the sign in cases of specific technical factors such as peristaltic movement of the surrounding bowel loops or close presence of bony structures. It is mandatory to consider positive the defect only in clear, not equivocal cases (Figs. 7.2 and 7.3).
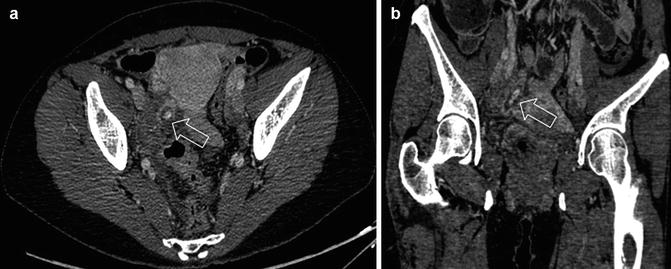
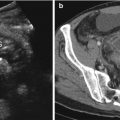
Fig. 7.2
MDCT axial (a) and MPR oblique (b) images show inflamed appendix with the presence of appendicolith inside and moderate amount of fluid in the lumen. Parietal enhancement defect can be appreciated (arrows) as a sign of perforation with associated fluid in the surrounding fat space

Fig. 7.3
Surgical finding from patient in Fig. 7.1. After appendicectomy wall necrotic area (arrow) corresponds exactly to not enhancing portion depicted at MDCT; extracted appendicolith (circle) causing appendicitis
Abscess presence: abscess is defined as a well-circumscribed fluid collection with thick wall showing positive enhancement. Gas can be seen in the context of the collection due to anaerobic bacterial presence or due to a direct communication with appendicular lumen. Many authors consider this sign the most specific for perforation diagnosis [2–12] (Fig. 7.4).
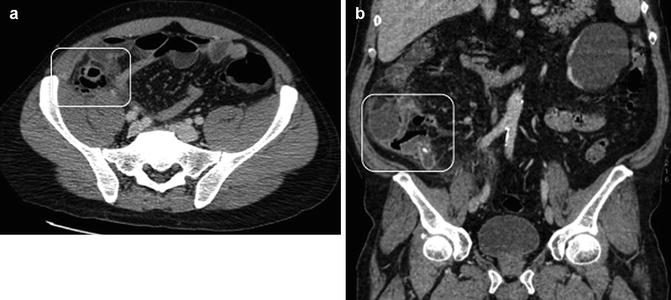
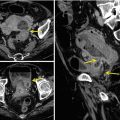
Fig. 7.4
MDCT axial (a) and MPR coronal (b) images show appendicular abscess with air-fluid level. In the rectangle (a, b) appendicolith obstructing the appendix valve and thick enhancing wall of the abscess can be appreciatedRelated posts:
 Role of Multidetector Row Computed Tomography in the Diagnosis of Gastroduodenal Perforation
Role of Multidetector Row Computed Tomography in the Diagnosis of Gastroduodenal Perforation
 Plain Film Signs of Pneumoperitoneum
Plain Film Signs of Pneumoperitoneum
 MDCT Imaging of Gastrointestinal Tract Perforation Due to Foreign Body Ingestion
MDCT Imaging of Gastrointestinal Tract Perforation Due to Foreign Body Ingestion
 Ultrasonographic Assessment of Gastrointestinal Perforation
Ultrasonographic Assessment of Gastrointestinal Perforation
 Acute Perforated Diverticulitis: Spectrum of MDCT Findings
Acute Perforated Diverticulitis: Spectrum of MDCT Findings
 Pneumoretroperitoneum: Imaging Findings
Pneumoretroperitoneum: Imaging Findings

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

