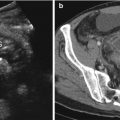
Fig. 11.1
Surgically confirmed right colon perforation caused by a salted codfish bone in a 56-year-old woman complaining with vague abdominal pain. Contrast-enhanced images (a–c: axial views, d: coronal thin-slab MIP) show tiny free air bubbles (arrowheads in a and b), thickening of the right colon wall with surrounding fat stranding (open arrow in c), and an endoluminal linear hyperdense structure indicative of foreign body (arrow in c), better appreciable on MIP reconstruction (arrow in d)
To be able to detect the FB, the radiologist has to keep in mind that besides an intraluminal or partial extraluminal location (Fig. 11.2) at the level of the perforated loop, it may lie free in the peritoneal cavity passing through the bowel wall. It means that we can find the FB far from the perforation site [3, 5].
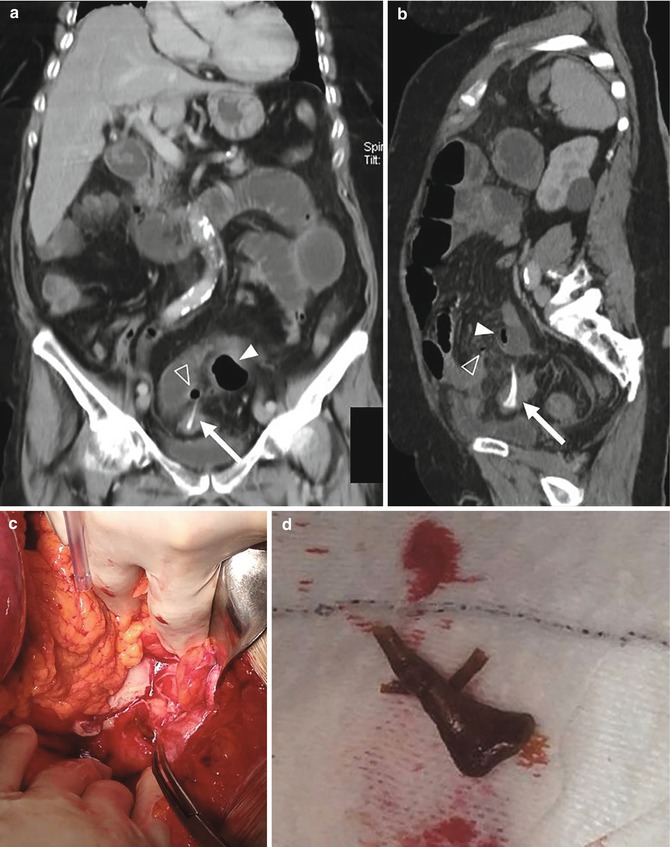
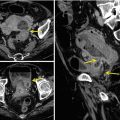
Fig. 11.2
Sigmoid colon perforation caused by a chicken bone in an 84-year-old woman with Alzheimer disease. CT images (a: coronal MIP; b: sagittal oblique MIP) show free air bubbles (open arrowheads in a and b) and a localized abscess (arrowheads in a and b) with a hyperdense foreign body through the sigmoid colon wall (arrows in a and b). These findings were confirmed by surgery (c, d: Courtesy of Prof. Felice Mucilli, Department of Biomedical Sciences, “G. d’Annunzio” University of Chieti, Italy)
We have to underline that, unfortunately, noncalcified wooden FBs, e.g., toothpicks, skewers, and chopsticks, may be missed even at an accurate inspection, owing to their isoattenuating appearance. Dry and fresh wood may respectively show air and water components, which are hardly distinguishable from the normal GI tract content (Fig. 11.3).
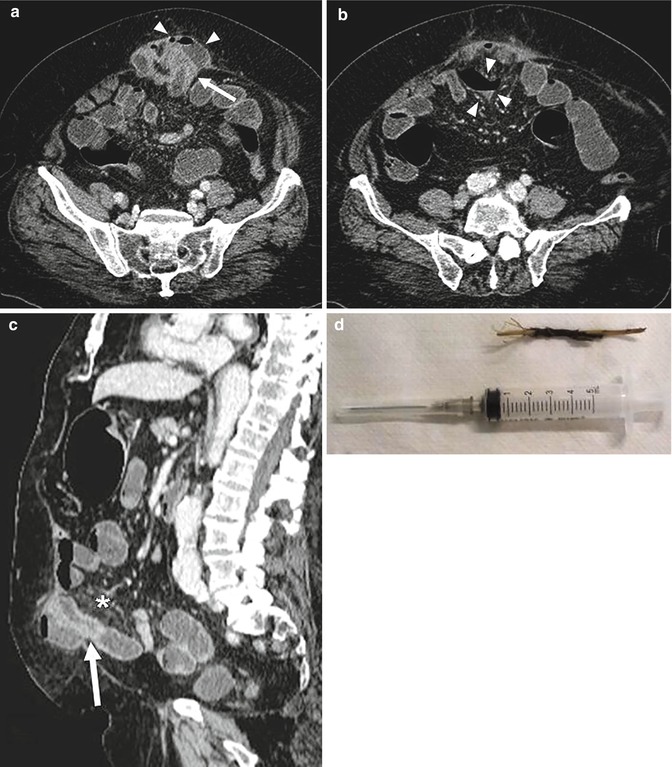
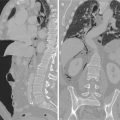
Fig. 11.3
 Role of Multidetector Row Computed Tomography in the Diagnosis of Gastroduodenal Perforation
Role of Multidetector Row Computed Tomography in the Diagnosis of Gastroduodenal Perforation
 Plain Film Signs of Pneumoperitoneum
Plain Film Signs of Pneumoperitoneum
 Imaging of Gastrointestinal Tract Perforation in the Elderly Patient
Imaging of Gastrointestinal Tract Perforation in the Elderly Patient
 Ultrasonographic Assessment of Gastrointestinal Perforation
Ultrasonographic Assessment of Gastrointestinal Perforation
 Acute Perforated Diverticulitis: Spectrum of MDCT Findings
Acute Perforated Diverticulitis: Spectrum of MDCT Findings
 Pneumoretroperitoneum: Imaging Findings
Pneumoretroperitoneum: Imaging Findings




An 81-year-old man presenting at the emergency department with acute abdominal pain and leukocytosis. Contrast-enhanced images (a, b: axial views, c: sagittal MPR) demonstrate dilated fluid filled small bowel loops and a postoperative ventral hernia including a small bowel loop that shows mural thickening (arrows in a and c) with adjacent mesenteric fat stranding (asterisk in c) and localized air/fluid collections (arrowhead in a and b). These findings were indicative of small bowel obstruction caused by the abdominal hernia, complicated with perforation. At surgery, a fragment of a wood skewer (d: Courtesy of Prof. Felice Mucilli, Department of Biomedical Sciences, “G. d’Annunzio” University of Chieti, Italy) was found within the perforated loop. The foreign body was not detectable on MDCT examination owing to its nature
Related posts:
Role of Multidetector Row Computed Tomography in the Diagnosis of Gastroduodenal Perforation
Plain Film Signs of Pneumoperitoneum
Imaging of Gastrointestinal Tract Perforation in the Elderly Patient
Ultrasonographic Assessment of Gastrointestinal Perforation
Acute Perforated Diverticulitis: Spectrum of MDCT Findings
Pneumoretroperitoneum: Imaging Findings
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
