Airway Diseases
10.1 Diseases of the Trachea and Mainstem Bronchi
10.1.1 Tracheal Stenosis and Stenosis of the Mainstem Bronchi
Benign tracheal stenosis usually occurs secondary to endotracheal tube cuff pressure alteration, typically in the middle trachea. The cuff pressure causes ischemic necrosis of the mucosa and subsequent fibrosis.1,2 This results in short stenosis of the tracheal lumen. In addition, several other causes of stenosis of the trachea or central bronchi are known.
Note 
Causes of tracheal stenosis2:
Intubation.
Penetrating or blunt trauma.
Postinfectious, especially in tuberculosis.
Anastomotic stenosis following lung transplant.
Crohn disease.
Sarcoidosis.
Granulomatous polyangiitis or Wegner granulomatosis.
Amyloidosis.
Tracheobronchopathia osteochondroplastica.
Perichondritis.
 |
Occasionally, tracheal stenosis can be identified on radiography. Computed tomography (CT) is able to reliably visualize stenosis even if, at times, this is not apparent on axial slices. Therefore, comparison of the tracheal lumen with adjacent and more distant slices is needed. Stenosis can be visualized more clearly on sagittal and paracoronal MPR (multiplanar reconstructions) or MinIP (minimum intensity projections) (▶Fig. 10.1),3 with the latter angled along the course of the trachea. Typically, the area of stenosis has a symmetrical, hourglass shape measuring up to 2 cm in length.
10.1.2 Tracheal Diverticula
Tracheal diverticula (paratracheal air cysts) are rare and usually asymptomatic incidental findings identified on CT scans.4 At times, chronic cough or recurrent infections, hemoptysis, stridor, or dyspnea may be observed. Occasionally, intubation difficulties lead to the diagnosis.5
Air accumulation in the superior thoracic aperture can sometimes be seen on radiography but CT is needed to reach the diagnosis (▶Fig. 10.2). A well-defined air accumulation is usually located right dorsal to the tracheal at the level of the superior thoracic aperture; an air-filled channel between the extraluminal air and the trachea can be identified.5
For differential diagnosis, other air-containing structures of the superior thoracic aperture must be taken into account, especially Zenker diverticulum of the esophagus, pharyngoceles, laryngoceles, apical lung hernias, bullae, and pneumomediastinum.4,5 An important differential criterion is detection of a communication between the trachea and diverticulum on CT.
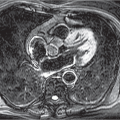
10.1.3 Tracheal Rupture
Traumatic tracheal rupture is rare but may occur secondary to chest trauma or iatrogenic tracheal injury during intubation. It usually affects the posterior tracheal wall, the softer membranous part.
 Fig. 10.2 Tracheal diverticulum. CT image. Retrotracheal, smoothly marginated air accumulation (arrow) right lateral to the esophagus (asterisk) with visible communication with the trachea (arrowhead). |
Tracheal rupture cannot be directly identified on radiography; indirect signs include mediastinal and cervical soft-tissue emphysema. CT is usually able to directly demonstrate the defect in the tracheal wall (▶Fig. 10.3). Furthermore, abnormal distension of a tracheal tube cuff is an indirect sign of tracheal rupture.6
10.1.4 Foreign Body Aspiration
Foreign body aspiration occurs predominantly in children younger than 6 years of age who are capable of aspirating the most diverse objects. In adults, foreign bodies are generally aspirated accidentally while ingesting food, usually chicken or fish bones, less commonly dentures.7 Predisposing factors include pathologic changes to the gastrointestinal tract, in particular esophageal stenosis, advanced age, mental retardation, or psychiatric disorders.
Note 
Foreign bodies are often found in the right lower lobe. Since the right mainstem bronchus has a steeper course than the left, most foreign bodies pass to the right side and, due to gravity, are dislodged more distal into the right lower lobe bronchus.
Larger, metallic objects are visible on radiography but other foreign bodies, including chicken or fish bones, almost never.7 CT is indicated if aspiration is suspected and no foreign bodies are radiographically seen. CT has very high sensitivity for detection of foreign bodies but does not have absolute specificity since, for example, endobronchial tumors can also mimic a foreign body (see ▶Fig. 10.5).
In almost half of cases, additional findings are identified on radiography, most commonly atelectasis, less often hyperinflation of parts of the lung due to a valve mechanism caused by the foreign body, or poststenotic pneumonia.8 Around 20% of all cases of foreign body aspiration have a normal radiograph. On CT, inflammatory changes to the bronchial wall manifest as wall thickening or luminal constriction, in particular in the case of a longstanding foreign body. Furthermore, in addition to inflammation, mucoceles or bronchiectasis is also often observed over time distal to the foreign body (▶Fig. 10.4).
 Fig. 10.3 Tracheal rupture. CT image. Gaping defect in the posterior tracheal wall (arrow) with massive mediastinal and softtissue emphysema. |
 Fig. 10.4 Aspirated chicken bone in the right lower lobe bronchus (arrow). CT, coronal image. Granulation tissue in the intermediate bronchus (arrowhead) and impaired aeration of the distal bronchus as well as bronchiectasis. |
 Fig. 10.5 Bronchial lipoma. CT image. Small, endobronchial mass of fat density (arrow) with distal atelectasis (arrowhead). |
10.1.5 Benign Tumors
Benign tumors of the trachea and the mainstem bronchi are much less common than malignant tumors. These are smoothly marginated, rounded tumors that are rarely more than 2 cm in size. Clinically, these generally manifest as stridor. The predominant findings on histology are papillomas, adenomas of the submucosal mucous glands, hamartomas, and lipomas.1
On CT these tumors present as polycyclic endoluminal masses that do not extend beyond the borders of the specific organ. Hamartomas, too, may also be seen to contain fat on CT, like pulmonary hamartomas.1 Likewise, lipomas characteristically exhibit fat-equivalent density on CT. Some endobronchial tumors cause atelectasis (▶Fig. 10.5).
10.1.6 Malignant Tumors
Malignant tumors of the trachea account for less than 1% of all thoracic tumors.9 The most common tumors are squamous cell carcinomas (▶Fig. 10.6), followed by adenoid cystic carcinomas (▶Fig. 10.7); less common are mucoepidermoid tumors and carcinoids.1 Clinically, only nonspecific early symptoms, such as dyspnea, stridor, hemoptysis, or dysphagia, are seen.
On radiographs, these tumors are rarely detected prospectively, although they can usually be identified retrospectively as constriction of the tracheal lumen.1 CT is able to visualize both the endobronchial tumor component and the tumor extension. The tumor is seen as a more or less circular area of enhanced thickening surrounding the tracheal or mainstem bronchial wall, with, in some cases, a pronounced endoluminal exophytic component (see ▶Fig. 10.6).
 |
10.1.7 Inflammatory and Other Systemic Diseases
Infections of the upper airways by human papillomaviruses cause papillomatosis. This disease usually affects children and is less common in adults. The usually multiple papillomas are classified as nonneoplastic lesions.2 Occasionally, they may even be seen on radiographs, and on CT they regularly manifest as endoluminal nodules in the trachea (▶Fig. 10.8).
Perichondritis (relapsing polychondritis) belongs to the collagen vascular diseases, in which recurrent inflammatory processes successively destroy the tracheal and bronchial cartilage clasps, leading to constriction of the airways. On CT, diffuse wall thickening and narrowing of the tracheal lumen can be identified. The destruction of cartilage clasps may also be visible on CT in cases with calcified cartilage.1
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


