planning and immediate treatment of complex cerebrovascular lesions. A significant level of arteriographic detail can be lost, however, due to relatively minor patient motion. Most children cannot adequately cooperate for cerebral arteriographic procedures; thus, deep sedation or neuroleptic anesthesia is an essential component of pediatric neuroangiography. While the decision to use conscious sedation or general anesthesia must be made on an individual basis, we prefer the use of general anesthesia in most cases, especially in preadolescent children. The sedation/anesthesia should be performed by an anesthesiologist with extensive pediatric experience and equipped with a complete set of pediatric cardiopulmonary life support and monitoring equipment. Monitored intravenous sedation may be substituted for general anesthesia during diagnostic angiography in the most cooperative patients. An exception to the use of anesthesia is the Wada activation test, which must be performed without sedation (9).
TABLE 12-1 Agents for Cerebral Embolization | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
of the more commonly used embolic materials. A complete review of the specific applications of these embolic agents is beyond the scope of this text.
hypertension, caused by high pressure and shear stresses from turbulent blood flow and consequent stenosis in draining veins (56,57). Thus, contrary to earlier descriptions, AVMs can have mass effect unassociated with hemorrhage. Rapid flow in the feeding arteries may result in the development of arterial aneurysms, both in the same distribution as classic berry aneurysms (circle of Willis) and in feeding arteries (pedicle and nidal aneurysms) close to the malformation (Fig. 12-1). In addition, varices (venous aneurysms) can develop upstream to the stenosis and cause hemorrhage if they rupture. As a result of all these factors, AVMs are the vascular malformations that most commonly cause neurological defects other than seizures, despite the fact that they are not the most common form of vascular malformations.
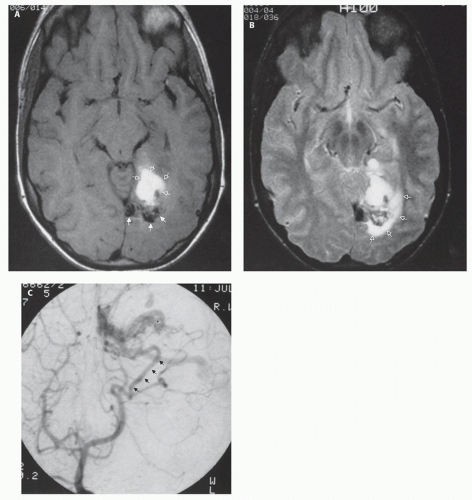 FIG. 12-1. AVM with hemorrhage. A. Axial T1-weighted image shows an area of high signal intensity in the left temporooccipital region (open arrows). This subacute hematoma lies directly ventral to a tangle of vessels (solid arrows), which presumably represents the nidus of the AVM. B. Axial T2-weighted image shows the tangle of vessels and hematoma. The area of high signal intensity (open arrows) dorsal and lateral to the tangle of vessels represents a small amount of edema. C. AP image from a left vertebral artery angiogram shows the vascular malformation being fed by the left posterior temporal artery (solid arrows). |
cause is probably cortical injury and gliosis from previous hemorrhage (62) or venous ischemia (63,64).
In larger malformations, the adjacent brain parenchyma can lose its ability to autoregulate; thus, staged palliative embolization is used to gradually re-establish regulatory control in the microcirculation and prevent the development of normal perfusion pressure breakthrough (86). In reducing the size and rate of flow through a malformation, improved obliteration of AVMs may be achieved by radiosurgery, although posttreatment evaluation is warranted.
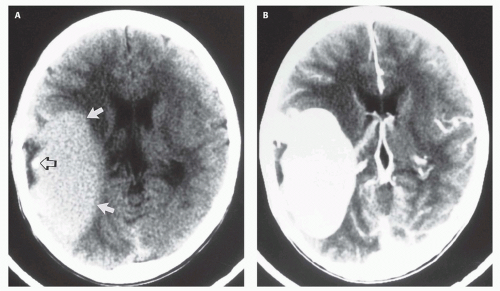 FIG. 12-2. A solitary arteriovenous connection (fistula). A. Axial noncontrast CT scan shows a large mass in the right sylvian area (solid arrows) that is hyperdense compared with brain parenchyma. A small focus of calcification (open arrow) is present within the mass. B. After infusion of iodinated contrast, the mass uniformly enhances. C. Coronal T1-weighted image shows a large amount of signal misregistration (arrows) from the mass in the phase-encoding direction. This phase misregistration artifact is essentially pathognomonic for a vascular lesion. D. Arterial phase image from a right internal carotid arteriogram, lateral projection, shows an enlarged Rolandic branch of the middle cerebral artery emptying into a large venous varix at the site of the solitary A-V connection. |
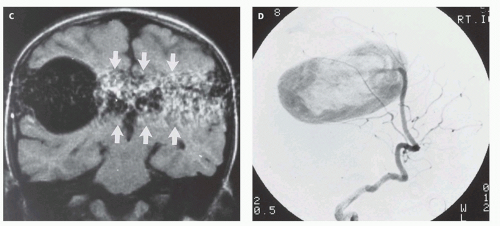 FIG. 12-2. (Continued) |
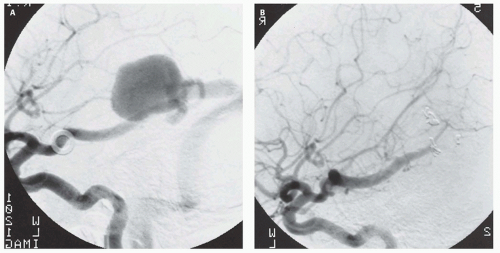 FIG. 12-3. A fourteen-year-old girl with severe unilateral headaches. A. Left internal carotid angiogram, lateral projection, shows a solitary fistula arising from the posterior temporal branch of the posterior cerebral artery. B. Same injection and projection, status post coil embolization, confirms complete closure of the fistula. |
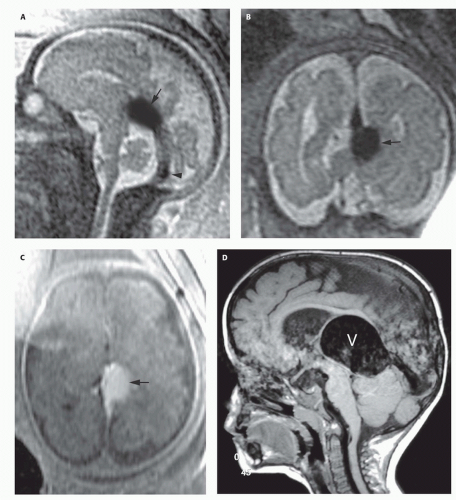 FIG. 12-4. Fetal and postnatal MRIs of vein of Galen malformations. A-C. Fetus of 29 week gestational age. Sagittal T2-weighted image (A) shows a large varix (black arrow) above the quadrigeminal plate cistern. The straight sinus (black arrowhead) appears normal or enlarged. Coronal T2 (B) and axial T1 (C) images show the large varix (black arrows). It appears hyperintense in (C) because of inflow of unsaturated protons on this spoiled gradient-echo image. E-H. A two-year-old boy with increased head circumference and Parinaud syndrome (paralysis of upward gaze due to compression of the brainstem tectum). D and E. Sagittal T1-weighted and axial T2-weighted images reveal marked enlargement of a central venous structure (the dilated median prosencephalic vein of Markowski, V) with hydrocephalus resulting from compression of the dorsal midbrain and cerebral aqueduct. F. Left vertebral artery injection, frontal projection in the arterial phase, demonstrates a mural-type vein of Galen malformation supplied by the collicular arteries through a single-hole fistula (curved arrow). G. Left vertebral injection, lateral projection in the late venous phase, shows to advantage the dilated prosencephalic vein of Markowski draining into a persistent falcine sinus. In these cases, the straight sinus is often absent, and it has been proposed that intrauterine thrombosis of the straight sinus results in the vein of Galen malformation. H. Left vertebral injection, frontal projection in the arterial phase following occlusion of the right and left collicular arteries, show complete occlusion of the malformation. The patient made an uneventful recovery and is now neurologically normal. |
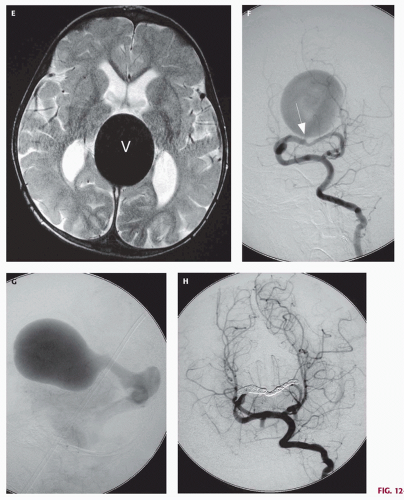 FIG. 12-4. (Continued) |
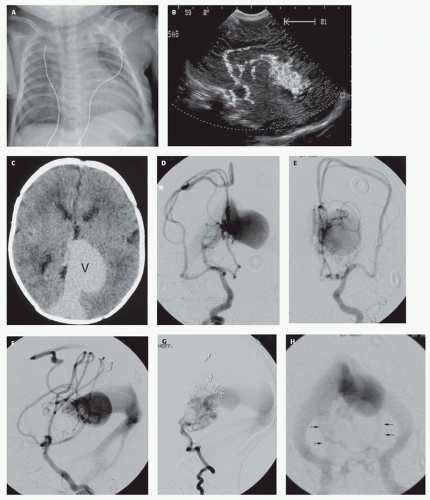 FIG. 12-5. Newborn with severe intractable congestive failure. A. Portable chest radiography demonstrates cardiomegaly and increased pulmonary vascular markings compatible with pulmonary edema due to high-output CHF apparent on physical examination. B. Transfontanelle color Doppler ultrasonography, sagittal plane, shows prominent anterior cerebral arteries in continuity with an enlarged deep central venous structure. C. Nonenhanced CT brain scan confirms the presence of markedly enlarged central venous structures (V), normal brain development, and the absence of hydrocephalus or hemorrhage. D-H. Complete cerebral arteriography in multiple projections demonstrates a choroidal-type vein of Galen aneurysmal malformation supplied by every major vascular distribution. Arteriovenous shunting converges upon a dilated primitive prosencephalic vein of Markowski continuous with a persistent falcine sinus. Presumably, due to the high-flow state, venous drainage includes persistent occipital sinuses (arrows, H). |
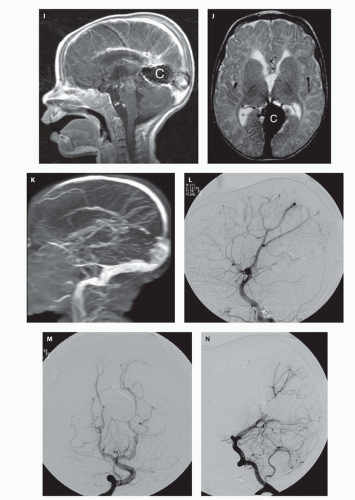 FIG. 12-5. (Continued) I-K. Following curative endovascular occlusion of the malformation, MRI brain scan demonstrates the coil mass (C), normal flow through the mature cerebral venous drainage system, the absence of cerebral infarction, and no hydrocephalus. Maximum intensity projection from 2D time-of-flight MR venogram shows intact superficial venous drainage. Drainage of the deep venous system is obscured by susceptibility artifact from the coils. L-N. Complete cerebral arteriography following both transarterial and transvenous embolization confirms complete absence of arteriovenous shunting and durable occlusion of this malformation. The child is now 4 years old, has a normal neurological exam, and meets all developmental milestones. Endovascular techniques are now the preferred treatment method for these lesions. |
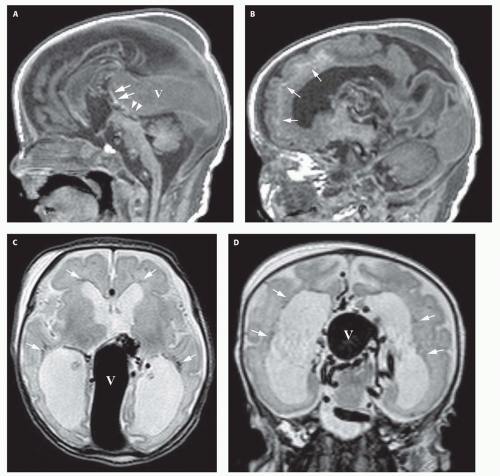 FIG. 12-6. Damaged brain in a vein of Galen malformation. This newborn presented with CHF. A. Sagittal T1-weighted image shows the large curvilinear varix (V) that compresses the aqueduct (white arrowheads), resulting in hydrocephalus, and anteriorly displaces the posterior wall of the third ventricle (white arrows). B. Parasagittal T1-weighted image shows abnormal subcortical hyperintensity (white arrows), indicating parenchymal injury. C and D. Axial (C) and coronal (D) T2-weighted images show the varix (V), multiple enlarged tortuous vessels around the midbrain and the varix, and abnormal hypointensity of the periventricular white matter (white arrows), indicating parenchymal injury/ necrosis. In addition, the ventricles are enlarged, likely secondary to a combination of hydrocephalus and loss of periventricular white matter volume. E. Average diffusivity (Dav) image shows reduced diffusivity (low signal intensity, arrows) in the posterior frontal periventricular and deep white matter. F and G. Partition image from time-of-flight MR angiogram (F) and maximum intensity projection from MR venogram (G) show the mural type of vein of Galen varix with enlarged anterior cerebral artery (large white arrowhead) and multiple branches and feeders from the posterior circulation (small white arrowheads) terminating in the varix (V). Note the enlarged emissary veins (white arrows in G) helping to shunt blood from the engorged intracranial venous system into extracranial veins. |
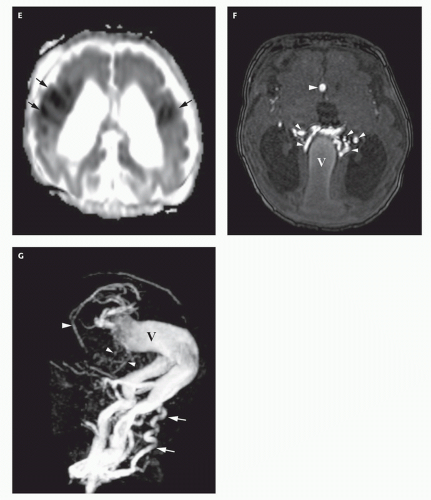 FIG. 12-6. (Continued) |
vessels. All five patients died during or shortly after the surgery. The subsequent eight patients underwent transvascular embolization techniques. Six of the eight survived while two died despite treatment (103). Of the survivors, one suffered a severe middle cerebral infarct resulting from an errant embolus. Another had a partial visual field deficit, presumably a result of ischemic damage secondary to the underlying disease. The remaining patients are neurologically and developmentally normal with marked reduction of the fistula flow following treatment. At long-term independent follow-up, 61% of patients who survived their initial presentation were neurologically normal or demonstrated only minor developmental delay (96).
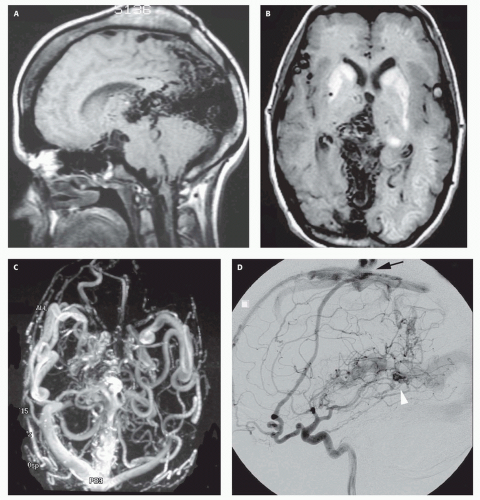 FIG. 12-7. A thirty-two-year-old woman with vein of Galen malformation and presenile dementia. A and B. Midsagittal T1-weighted and axial T2-weighted images show severe calvarial thickening from chronic anticonvulsant use and extensive flow voids along the posterior falx cerebri and tentorium cerebelli, surrounding the primitive median prosencephalic vein and persistent falcine sinus. The basal ganglia hyperintensity probably represents injured, calcified tissue from chronic venous hypertension. C. 3D Phase-contrast MRA illustrates the dramatic increase in the size of intracranial blood vessels caused by the congenital vein of Galen malformation and subsequent recruitment of additional blood supply from all vascular distributions. D-F. Left internal carotid, external carotid, and vertebral injections, lateral projection in the arterial phase, define the recruitment of blood supply to the fistula from all vascular distributions. Chronic venous hypertension has engendered development of several independent and noncontiguous fistulas of the superior sagittal sinus (black arrow) and falx cerebri (white arrowhead). |
 FIG. 12-7. (Continued) |
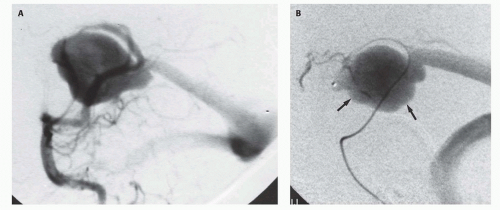 FIG. 12-8. A three-month-old infant presents with Parinaud syndrome (paralysis of upward gaze) and an enlarging head circumference. A. Left vertebral artery injection, lateral projection, demonstrates a mural type vein of Galen malformation with two large-caliber connections. B. A microcatheter has been navigated into the fistula site and contrast injected delineating the draining prosencephalic vein (arrows). C-E. Superselective injection following embolization with microcoils demonstrates complete occlusion of the fistula. Note preservation of all normal vessels, including the choroidal vessels, parietooccipital branches, and connection to the distal splenial and pericallosal artery. |
If the diagnosis is established prenatally, the delivery should be performed at an institution offering endovascular techniques to palliate the patient should intractable CHF develop. Severe heart failure in utero can result in polyhydramnios and hydrops fetalis, which can be an indication for induced delivery. Close coordination among the obstetricians, neurointerventionalists, neonatologists, and neurosurgeons is essential to optimize planning. Baseline ultrasonography with color flow Doppler should be performed to serve as a baseline for blood flow in evaluating the results of the endovascular techniques. If possible, umbilical arterial and venous catheters should be placed at the time of delivery to allow repeated vascular access for both diagnostic and therapeutic procedures. These indwelling catheters obviate the necessity for repeated femoral punctures in the fragile neonatal femoral artery. A CT or MRI should be performed to assess any parenchymal damage already produced by the congenital fistula, disclose hydrocephalus, which may require ventriculoperitoneal shunting, and serve as a baseline.
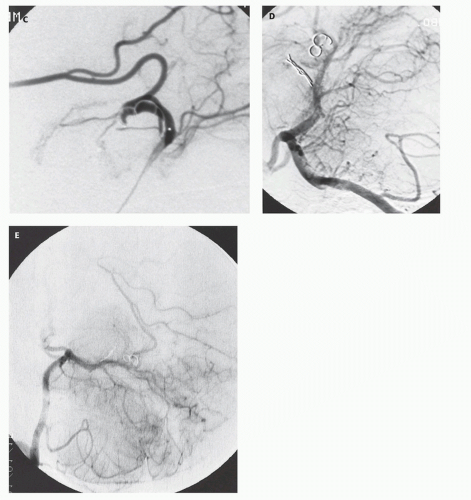 FIG. 12-8. (Continued) |
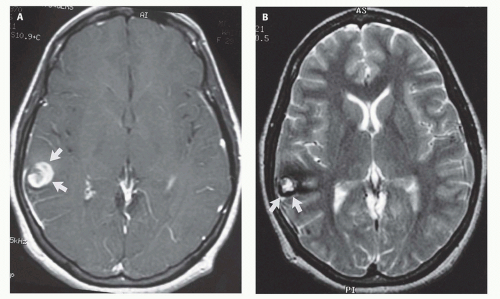 FIG. 12-9. Cavernous malformation. A and B. Child with epilepsy. Contrast-enhanced axial T1-weighted image (A) shows an area of mixed signal intensity surrounded by a low-intensity rim (arrows) in the right posterior frontal lobe. This is the classic appearance for cavernous malformations. Axial T2-weighted image (B) demonstrates T2 hypointensity compatible hemosiderin (arrows) from prior hemorrhage surrounding an irregular hyperintense core. |
question, decompression for mass effect causing neurological deficits, and intractable or chronic seizures (121).
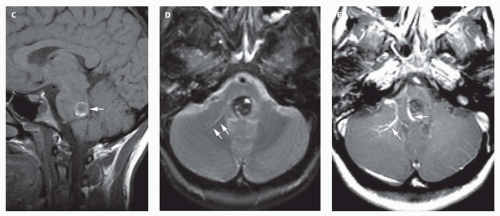 FIG. 12-9. (Continued) C-E. Child with new ocular dysmotility. Axial T1-weighted image (E) shows a hyperintense rim in the dorsal pons (white arrow). Axial T2-weighted image (F) shows the lesion to be heterogeneous, mostly hypointense with areas of intermediate and marked hyperintensity. A large vein (arrows) is located in the left cerebellar hemisphere; note the hyperintensity adjacent to the hypointense vein, due to mismapping of signal from slow flow. Postcontrast T1-weighted image (E) shows two large developmental venous anomalies (arrows), with one coursing directly to the right of the cavernoma. |
TABLE 12-2 Categories to Characterize Cavernous Malformations Using Spin-echo Sequences on MRI Correlated With Surgical Outcomes | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
vein, the lateral transpontine vein, or the vein of the lateral recess of the fourth ventricle (127). The parietal lobe is also a fairly common site, accounting for about 15% of venous malformations; the temporal and occipital lobes are less common locations (126,127,128,129). If longstanding venous ischemia has been present, the region of brain that has been drained by the venous malformation may become atrophic and calcified. In approximately 5% of these cases, there may be complicating features such as aneurysms or transitional features including arteriovenous shunting that is the hallmark of a pial AVM. In patients with progressive neurological symptoms or hemorrhage, catheter angiography may be useful to evaluate for high-risk features (130).
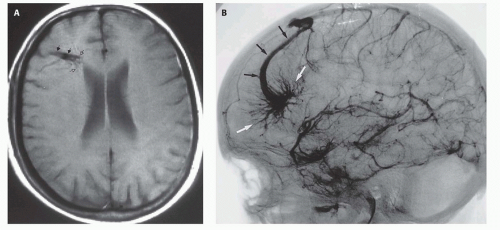 FIG. 12-10. Developmental venous anomaly. A. Axial T1-weighted image shows a tuft of vessels (open arrows) feeding into a curvilinear vascular channel (solid arrows) that drains into the superior sagittal sinus (not seen on this image). This appearance is characteristic of developmental venous anomalies. B. Venous phase angiogram, lateral projection, from a right internal carotid artery injection. The tuft of vessels (white arrows) is seen to form a curvilinear venous channel (black arrows) that drains into the superior sagittal sinus. The findings are identical to what was seen on the MR study. |
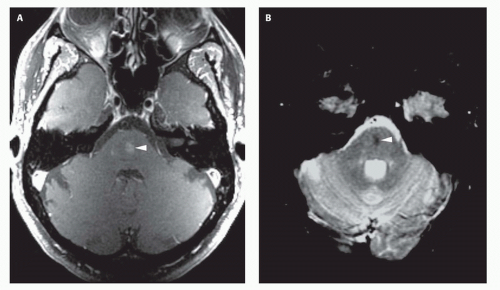 FIG. 12-11. Capillary telangiectasia. A. Axial postcontrast T1-weighted image shows a small area of enhancement (arrowhead) in the middle of the pons. B. Axial T2*-weighted gradient-echo image shows hypointensity of the enhancing region in the central pons (arrowhead), indicating the presence of chronic hemorrhage and establishing the diagnosis of capillary telangiectasia. |
hypointensity is typically seen on gradient-echo images (Fig. 12-11) (131), presumably secondary to the presence of slowly flowing, deoxygenated blood within the vessels (132).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


