Anomalies of the Cerebral Vasculature: Diagnostic and Endovascular Considerations
Anomalies of the Cerebral Vasculature: Diagnostic and Endovascular Considerations
Steven W. Hetts
Philip M. Meyers
Van V. Halbach
A. James Barkovich
Introduction
Cerebrovascular disease is uncommon in children and adolescents. In children under the age of 15, the average annual incidence of cerebral vascular disease unrelated to trauma or infection ranges 2.5 to 3.1 per 100,000 population (1,2,3,4). Pediatric vascular disease can be grossly divided into occlusive vascular disease and causes of intracranial hemorrhage. Occlusive vascular disease and its imaging manifestations were discussed in Chapter 4. This chapter discusses cerebral vascular anomalies and cerebral vascular disorders amenable to endovascular intervention.
Vascular malformations are the cause of nearly all nontraumatic intracranial hemorrhages in children beyond the neonatal stage. Tumors, the next most common cause of hemorrhage, occur far less frequently (5,6). Therefore, any child presenting with spontaneous intracranial hemorrhage should be evaluated for child abuse (see Chapter 4) and for vascular malformations.
The treatment of pediatric cerebrovascular disease continues to advance rapidly. Endovascular techniques now permit palliation or cure of many disease entities. In VOGMs, for example, morbidity and mortality have been significantly reduced using endovascular techniques compared with conventional surgery. Consequently, a premium is placed upon the rapid recognition of treatable illness to facilitate prompt and appropriate intervention. This chapter discusses pediatric cerebrovascular disorders, with consideration toward endovascular management when indicated.
Technical Considerations in Pediatric Neuroangiography and Intervention
Although computed tomographic angiography (CTA) and magnetic resonance angiography (MRA) can answer many questions about the vasculature of the brain, head, and neck, catheter angiography remains essential to careful analysis of disorders of the cerebral vasculature. In experienced centers with dedicated neuroangiographers, cerebral angiography is a very safe procedure, with low morbidity (7,8). Modern fluoroscopic equipment permits high-resolution biplane digital subtraction arteriography. High spatial resolution, high-speed real-time image acquisition, and high-resolution roadmapping facilitate surgical planning and immediate treatment of complex cerebrovascular lesions. A significant level of arteriographic detail can be lost, however, due to relatively minor patient motion. Most children cannot adequately cooperate for cerebral arteriographic procedures; thus, general anesthesia is essential component of pediatric neuroangiography. While the decision to use conscious sedation or general anesthesia must be made on an individual basis, we prefer the use of general anesthesia in most cases, especially in preadolescent children. The sedation/anesthesia should be performed by an anesthesiologist with extensive pediatric experience and equipped with a complete set of pediatric cardiopulmonary life support and monitoring equipment. Monitored intravenous sedation may be substituted for general anesthesia during diagnostic angiography in the most cooperative patients. An exception to the use of anesthesia is the Wada activation test, which must be performed without sedation (9).
Indications
The indications for cerebral arteriography in the pediatric population continue to evolve. Many clinical questions can now be adequately addressed using noninvasive methods including magnetic resonance imaging (MRI), ultrasound, or computed tomography (CT). An effort to avoid exposure of a child to radiant energy is important according to the ALARA principle for use of medical radiation (10,11,12); therefore, MRI/MRA and ultrasound are used whenever possible, and radiation dose is kept as low as possible, while still obtaining diagnostic quality exams, when CT and radiographs are acquired.
X-ray dose limitation during pediatric neurointerventional procedures has become an area of significant attention in the past few years. Orbach and colleagues have estimated that long neurointerventional radiology procedures (e.g., embolization of an intracranial arteriovenous fistula) can result in brain-absorbed doses in young children such that their lifetime risk for CNS tumors is significantly increased (13). For children who are already at an increased risk for cancers, such as infants with ocular retinoblastomas due to loss of the Rb tumor suppressor gene, ALARA principles are even more important. Working with a medical physicist to optimize imaging parameters and technique settings for pediatric neurointerventions, as well as emphasizing the use of roadmap techniques over DSA techniques whenever possible, can markedly reduce radiation dose to the child (14).
The most common indications for cerebral arteriography are unexplained cerebrovascular accident (CVA); posttraumatic neurological deficit, stroke, or hemorrhage; functional neurologic testing prior to epilepsy surgery using the Wada technique; evaluation and treatment of craniofacial and cerebrovascular anomalies; and preoperative embolization of vascular neoplasms. The number of diagnostic pediatric cerebral arteriograms has diminished as x-ray CT techniques (including helical CT, CT angiography, and CT perfusion), MRI and MRA, and transcranial Doppler (TCD) have evolved. Meanwhile, marked improvements in microsurgical and endovascular techniques require information for surgical planning that catheter arteriography alone can provide. It is possible that diagnostic catheter arteriography may ultimately be left to those centers where therapeutic procedures are performed, if necessary. In this way, the optimal arteriographic series to suit the needs of the interventional neuroradiologist or neurosurgeon can be obtained.
Preprocedural Planning
Catheter angiography is an invasive procedure; thus, preoperative planning, as for any surgical procedure, is critical. The indications must be reviewed in light of all previous imaging studies, prior surgical procedures, and evolution of the anatomic pathology. Discussion among the angiographer, referring clinician, consultants, the patient, and the patient’s family should result in consensus on goals and expectations for treatment. It is important that the angiographer obtains a tailored history and physical examination in order to identify specialty-specific factors such as allergies, medications, and renal or hematologic diseases that could delay or alter performance of the angiogram. Preprocedural physical examination including neurologic evaluation is also important so that any changes during the procedure can be quickly recognized and expeditiously treated. Evaluation of the extremities, including lower extremity pulses, is relevant to selection of a site for vascular access. Unique risks to pediatric angiography are the development of leg length discrepancy and claudication due to injury of the femoral artery and femoral capital necrosis due to injury of the foveolar artery. Other complications of diagnostic angiography include stroke, iodinated contrast reaction, renal failure, and puncture site hematoma (15,16,17,18). In general, catheter cerebral arteriography can be performed with a minimum of risk (0.3%) at experienced centers (8).
Prior to embolization of an arteriovenous malformation (AVM), an echocardiogram possibly including a “bubble test” is warranted to evaluate for the presence of right-to-left intracardiac shunts. It is possible for embolic materials or thrombus to pass through an AVM into the normal venous drainage and the right side of the heart. Ordinarily, these small emboli will be filtered by the pulmonary vascular bed and in small numbers without any clinically significant consequences. Intracardiac shunts, common in pediatric patients with certain cerebrovascular malformations, could cause such emboli to pass from the right heart into the left heart and recirculate into the arterial system. The presence of intracardiac shunts means that great care must be undertaken during the embolization procedure to avoid the use of agents likely to pass through the cerebral AVM with resultant embolization to the systemic circulation (19). Pulmonary arteriovenous shunts are also a clinical concern in young patients with hereditary hemorrhagic telangiectasia syndrome (HHT, also known as Osler-Weber-Rendu disease). In such patients, assiduous attention to eliminating all air from venous access lines is required in order to lower the risk of air embolism-induced stroke. Clear communication with practitioners providing anesthesia or intravenous medications preoperatively, intraoperatively, and postoperatively is imperative. The use of air filters on intravenous lines (e.g., 0.22 micron filters) can also reduce the risk or air embolism in patients with intracardiac or pulmonary shunts (20).
The importance of preoperative preparation in regard to the pediatric patient cannot be overemphasized (21,22). Medications (including iodinated contrast) can cause dramatic shifts in intravascular fluid volume and vasomotor tone. An ill child may appear hemodynamically stable but, in actuality, may be exerting maximal physiological mechanisms to maintain blood pressure, systemic, and cerebral perfusion. Administration of sedatives, anesthetics, or vascular contrast can cause hemodynamic collapse in a volumedepleted child. As children undergoing cerebral arteriography may have elevated intracranial pressure (ICP), adequate ventilation is essential to prevent buildup of CO2 (and consequent elevation of ICP) that could result in herniation syndromes or hinder cerebral perfusion. Occasionally, manipulation of ventilation rate and blood pressure may be necessary to modulate arterial carbon dioxide levels and vasomotor tone. Changes in the pCO2 can be used to enhance cerebral arteriographic resolution, to reduce the volume of contrast, or to assist distal microcatheter manipulation (23). However, in children with suspected ischemic stroke, especially in the setting of moyamoya disease, blood pressure should be supported while maintaining normal pCO2. These children will stroke if overventilated. Therefore, the pCO2 should only be manipulated by highly experienced personnel and in the presence of ICP monitoring in order to prevent cerebral hypoperfusion and herniation syndromes. Careful monitoring during the administration of sedative medications and vascular contrast is essential.
Fluid and Contrast Limitations
To limit osmotic fluid shift and to reduce the incidence of contrastinduced renal injury, contrast dose (300 mg iodine/mL nonionic contrast) should not exceed 6 cc/kg. For routine digital subtraction angiography, contrast can be diluted by 50% (to 150 mg iodine/mL) if modern fluoroscopic equipment is used. Modern “biplane” neuroangiography equipment allows acquisition of arteriographic series in two projections simultaneously. Evaluation of high-flow arteriovenous shunts may require use of full-strength contrast. In order to get the most angiographic information out of each intra-arterial contrast injection in babies with high-flow intracranial shunts, in addition to standard “first-pass” arterial and venous phase images of the brain, the practitioner can continue to acquire angiographic images through the “second-pass” of contrast once it has gone through the patient’s heart and is now being pumped (albeit in dilute form) through both vertebral arteries and carotid arteries back through the entire brain. Secondpass angiography provides an overview of the relationship between the primary feeders of a vascular malformation and other cerebral vessels. Each catheter, including access sheaths, must be continuously flushed with heparinized saline (1000 units heparin/L) through a flow-regulated system with at least 3 cc/h. However, overly exuberant flushing can cause fluid overload and congestive heart failure (CHF) in small children or children with renal impairment. The anesthesiologist should be informed of the total fluid infusion volume and rate of fluid administration through all catheters. Limitations to contrast and fluid load are a common indication for staging embolization procedures over several sessions in very young children—for example, neonates with high-flow VOGMs—with time in the ICU in-between embolization sessions during which fluid and contrast can be removed either naturally through urinary excretion or, in the sickest children, through dialysis.
Vascular Access
Arterial access is the first critical step in performance of any pediatric neuroangiographic procedure. A child’s vessels are small in caliber, prone to spasm, highly mobile, and elastic. These factors often conspire to make arterial access a daunting challenge. Use of real-time ultrasound guidance during micropuncture access to the femoral artery has made a femoral artery puncture significantly easier in the past decade than in prior eras, however. Improper technique can result in laceration or thrombosis of the vessel. Arterial cannulation is facilitated by extension of the legs and elevation of the pelvis to straighten the common femoral artery. Following induction of general anesthesia, systemic blood pressure is often reduced, and manual palpation of the femoral and pedal pulses may become difficult. Marking the skin over the femoral puncture site as well as the foot over the dorsalis pedis and posterior tibialis pulses prior to anesthetic induction can facilitate cannulation and postoperative patient assessment. Proper positioning and padding of pressure points is necessary, particularly in infants and small children. Use of a Micropuncture set and a 3 or 4 French access sheath-catheter system will help to reduce local trauma at the puncture site. Analogous to the concept of ALARA in x-ray dose limitation, keeping the caliber of vascular sheaths placed in the arteries of children as small as possible is key to lowering the risk of arterial injury, access site thrombosis, and distal arterial embolization. Although rare, and often difficult to attribute to a particular angiographic procedure, the potential for adult leg length discrepancy as a late complication of transfemoral angiography in very young children whose lower extremity blood flow could be compromised by femoral artery occlusion or stenosis, should be mentioned to parents during informed consent discussions prior to angiography. It can also be helpful intraprocedurally to have pulse oximeters placed on both great toes: reduced flow to the foot on the side of femoral artery access can be followed intraprocedurally and may be managed with administration of nitropaste, another vasodilating medication, or heparin after access has been achieved.
Systemic heparinization (70 units/kg) during catheterization may also reduce the risk of thrombosis. Assessment of anticoagulation status in the angiography suite is rapidly performed using the activated clotting time (ACT). Depending upon the indication for angiography and other mitigating factors, an ACT 2-3X baseline value is considered therapeutic. In the presence of a recent cerebral hemorrhage or surgical procedure, anticoagulation may be contraindicated. A lower level of anticoagulation for interventional procedures should be considered, if necessary. Following removal of the femoral sheath, access for subsequent arteriographic procedures should alternate between the right and left femoral arteries. In special circumstances, such as neonatal arteriography, the umbilical artery and vein readily provide vascular access for catheter systems sized up to 5 French. If so requested, the neonatology service will maintain umbilical catheters to permit arterial and venous access for endovascular procedures. Umbilical artery access is particularly helpful for the treatment of high-flow intracranial lesions in neonates, as it generally allows multiple embolization sessions with less chance of access site scarring than femoral artery access (24).
Catheter Choice
The choice of angiographic catheter depends upon the application and patient size. The smallest diameter catheter that readily permits diagnostic arteriography is a 3 French catheter, which is used in neonates and infants. Smaller diameter catheters do not generally allow sufficient injection rate for routine arteriography. Slightly larger (4 French) catheters can be used in older children and provide greatly improved injection rates due to decreased flow resistance. Diagnostic catheters with an intrinsic hockey-stick tip-shape can often be custom-shaped using steam heating to reduce their angulation and allow them to sit less traumatically in the relatively straight cervical vessels of small children without high-flow lesions. For children with high-flow lesions, cervical vessels are often markedly tortuous and more angulation of catheter tips can be advantageous. Although not angulated, the same distal access catheters that have become widespread as intermediate support catheters during stroke intervention in the last decade have also gained popularity as access catheters for intracranial interventions in children either in combination with a short vascular access sheath or as a stand-alone. Manipulation of these catheters without a sheath at the access site with attendant vasospasm and potential damage at the access site, however, may limit their utility in cases wherein extensive navigation between multiple arterial pedicles is necessary. The length of distal access catheters may also limit their utility in small children, as the long segment of these catheters external to the patient needs to be stabilized in order to prevent extracorporeal torque dissipation during catheter navigation. Standard microcatheters can be advanced either through a 4 French diagnostic catheter platform in the cervical vessels or directly through a 4 French access sheath in the femoral artery without coaxial passage into the craniocervical region. Older children and adolescents will tolerate the use of the 4 to 6 French catheter systems commonly used in the adult population. Percutaneous access sheaths are used routinely in our practice to facilitate catheter exchange and to reduce trauma at the puncture site.
Endovascular Occlusion
The purpose of interventional neuroradiology is the minimally invasive treatment of vascular lesions. The fundamental principle of this treatment is occlusion of pathological vascular channels to improve the patient’s neurological or cardiovascular condition. Embolization, or endovascular occlusion, requires placement of the tip of a microcatheter in proximity to the abnormal vessels so that these channels can be selectively occluded, sparing normal or other needed vessels. Recent and ongoing developments in catheter technology allow careful and precise placement of embolic materials within the abnormal vascular channels while avoiding embolization of the normal adjacent vessels. A number of embolic materials are currently in use, and many more are under development or employed in clinical practice outside the United States. Table 12-1 lists some characteristics of some of the more commonly used embolic materials. A complete review of the specific applications of these embolic agents is beyond the scope of this text.
Table 12-1 Selected Agents for Neurovascular Embolization
Agent
Physical State
Manufacturer
Application
Size
Permanence
Polyvinyl alcohol
Particulate
Cordis, Target
Preoperative tumor, AVM embolization
45-1000 µm, calibrated sizes
++
Embospheres
Particulate
Biosphere Medical
Tumor embolization
40-1200 µm, calibrated sizes
+++
Platinum coils
Metallic Coil
Several
Tumor, AVM
Multiple
++++
Detachable platinum coils
Metallic Coil
Several
Aneurysm, AVM
Multiple
++++
Balloons
Latex
Balt
Fistula (not FDA approved in the USA)
Multiple
+++
Cyanoacrylate
Liquid Adhesive
J&J, Codman
AVM, Fistula
N/A
++++
Ethylene vinyl copolymer
Liquid Precipitate
Medtronic
AVM, Fistula
N/A
+++
Ethanol
Sclerosant
Abbott
Fistula, AVM
N/A
++++
Ethanolamine oleate
Sclerosant
Questcor
Hemangioma, venous, and lymphatic malformations
N/A
++++
Sodium tetradecyl sulfate
Sclerosant
Bioniche
Venous and lymphatic malformations
N/A
++
Doxycycline
MMP modulator
Several
Lymphatic malformations
N/A
++
Postprocedural Patient Care
At completion of an arteriographic procedure, the femoral access catheter must be removed and the puncture site must be manually compressed. Arterial closure devices generally require an artery that is at least 5 mm in diameter to be deployed safely; these devices are also currently not approved for use in children in the United States. Ideally, the catheter is removed while the patient is still under anesthesia to assure optimal control of the puncture site. Continuous Doppler monitoring of the pedal pulses is recommended to prevent excessive pressure with inadvertent thrombosis of the femoral artery during manual compression. Hemostasis is usually attained within 15 minutes in a patient with normal coagulation parameters. An anticoagulated patient may require the administration of protamine sulfate (10 mg protamine per 1000 units of active heparin in the blood) to reverse the effects of heparin prior to removal of the access catheter. Coagulopathy for other reasons may require administration of blood products or synthesized hemostatic factors. With an ACT below 180 seconds, it is usually possible to obtain arterial hemostasis. Thereafter, the patient should be closely monitored for several hours for evidence of puncture site bleeding, subcutaneous hematoma, or loss of distal pulses. Due to often exuberant arterial vasospasm, delayed access site bleeding appears to be less common in children than in adults. In younger children, keeping a common femoral artery puncture site immobile for several hours can be challenging. One technique to encourage the child not to bend at the hip is to use a soft knee brace or knee immobilizer applied loosely to the knee on the side of the arterial puncture. As most children tend to flex at the knee at the same time they flex at the hip (“frog-leg” movement), keeping the knee straight often reduces the urge to flex at the hip too.
Intracerebral Hemorrhage in Children
In contrast to adults, intraparenchymal hemorrhage is at least as common as ischemic stroke in children, and it is an important cause of morbidity and mortality (25,26,27). Trauma is the most common cause of intraparenchymal hemorrhage; the cause can be deduced from history or external evidence in these patients. Vascular malformations seem to be the most common cause of spontaneous cerebral hemorrhage in children, with true AVMs accounting for about 25% and cavernous malformations about 20% (28). Although AVMs have commonly been thought to have a higher hemorrhage rate in children than in adults, recent analysis suggests that second hemorrhages are less frequent in children than in adults, although treatment bias may affect that statistic (29). Tumors account for about 10% (usually ependymoma or highgrade glioma or PNET) and venous sinus thrombosis for another 10% (28,30); venous thrombosis seems more common in infants and neonates (30,31,32). Aneurysms are an uncommon cause, accounting for less than 5% (28,33). Most of the remaining cases are the result of systemic disease, such as infection, leukemia, or severe thrombocytopenia (28,34).
CT remains the primary imaging modality in the initial diagnosis of intracranial hemorrhage. After the presence of hemorrhage has been established, MRI with MRA and MRV can often establish the cause of hemorrhage. MR with and without contrast may reveal enhancing tumor, if present, and may show anatomically remote cavernomas or an adjacent developmental venous anomaly (DVA) that will allow a diagnosis of cavernous malformation. Large aneurysms or vascular malformations will also be evident by MR or MRA. Venous thrombosis can be detected by hyperintense signal in the vein on T1-weighted images or on MRV (more discussion of venous thrombosis is found in Chapters 4 and 11). If the MR is unrevealing, diagnostic catheter angiography becomes an important tool to look for small vascular malformations (35).
Intracerebral Vascular Malformations
Intracerebral vascular malformations (AVMs) are malformations of the cerebral vasculature that may involve arteries, capillaries, or veins. Although a few reports of familial vascular malformations have been reported (36), the majority are sporadic. Hereditary hemorrhagic telangiectasia syndrome (HHT, also known as Osler-Weber-Rendu disease) is the most common heritable cause of brain AVM; if multiple brain AVMs (almost pathognomonic of HHT) are present on imaging studies, they should prompt a workup for that autosomal dominant disease (20,37). Pathologically, vascular malformations have been subdivided into four groups. In McCormick’s series of 248 children with vascular malformations, arteriovenous malformations were found in 12%, developmental venous anomalies in 62%, cavernous malformations in 8%, and capillary telangiectasias in 18% (38). Of 417 children with intracranial arteriovenous shunting malformations seen at UCSF between 1986 and 2010, 74% had nidus AVMs, 6% had non-Galenic pial arteriovenous fistulas (NGAVFs), 10% had dural arteriovenous fistulas, and 9% had VOGMs (39,40,41,42). VOGMs, a type of AVM specific to neonates and infants, and facial AVMs are discussed separately, as special cases of AVMs.
Arteriovenous Malformations
Description and Causes
AVMs are compact collections of abnormal, thin-walled vessels (most commonly called the nidus, this is the true malformation) that connect dilated arteries to veins without an intervening capillary network. These persistent primitive connections between arteries and veins are formed during the late somite stages of the fourth embryonic week; they develop from the sinusoidal vascular network that perfuses the early developing telencephalon. The absence of capillaries produces a low resistance shunt, which results in rapid arteriovenous shunting within the malformation.
Patients with cerebral AVMs most commonly present as a result of spontaneous intracerebral hemorrhage (up to 61% of cases) during late childhood (43) or as a young adult (44), but affected patients can present at any age or, rarely, with seizures (29,45,46). Intraparenchymal hemorrhage can cause significant injury at any age, with 30% to 50% neurological morbidity and 10% mortality (47). Consequently, a premium has been placed upon identification and treatment of AVMs at major neurosurgical centers throughout the world.
The prevalence (total number of cases in a population at a given time) of AVMs has been estimated in autopsy series between 0.06% and 0.11% (44,48). Symptomatic AVMs were detected in 1 per 100,000 person-years, and prevalence was inferred from the incidence data to be less than 10 per 100,000 in a US population study (49,50) and 5 per 100,000 in Australia (51). Thus, although the precise numbers are not known, it seems that a significant percentage of AVMs become symptomatic during the average human lifetime, usually due to hemorrhage (44,51,52).
The vascular channels of AVMs that develop instead of normal capillaries are characterized by fibrointimal thickening and elastic tissue disorganization. These features probably take time to develop, and thus, classic brain AVMs (those with the classic tangle of vessels that compose the nidus) are not typically seen before birth or in early infancy. Flow-related angioarchitectural features in pediatric AVMs also appear to take time to develop postnatally: there is a paucity of feeding artery aneurysms and venous outflow stenosis in young children with AVMs (Fig. 12-1) as compared to older children and adults (39). No classic AVMs have been described prenatally, although several fetal cases with NGAVFs (direct connections between artery and vein without the tangle of abnormal vessels) have been identified (47). In neonates, AVMs are generally seen as direct arteriovenous communication without intervening nidus. Thus, AVMs seem to evolve, not becoming fully developed until later in life (53). De novo development of AVMs has rarely been documented in children or adults (54). Although most brain AVMs are thought to be congenital, a growing number of case reports of de novo brain AVMs has challenged this view in the past decade (55,56,57). In these apparent de novo cases in children and adults, there may well have been microscopic arteriovenous abnormalities below the detection threshold of MRI since early in development, but only later in life did the abnormality enlarge enough to be seen on noninvasive imaging.
No definite genetic linkage has been identified with the exception of Rendu-Osler-Weber (58) and Wyburn-Mason syndromes (59). Dysautoregulation of vascular growth factors has been implicated in the subsequent development and maturation of the vascular malformation (60).
AVMs often increase in size with age, as a result of increase in size of the nidus and progressive dilation of the feeding arteries and draining veins. Astrogliosis and atrophy are often seen in surrounding brain tissues. This was at one time thought to be a consequence of low resistance shunting of blood through the nidus, causing parenchymal hypoperfusion (vascular steal). Others suggest that edema and subsequent parenchymal injury results from venous stenosis/venous hypertension, caused by high pressure and shear stresses from turbulent blood flow and consequent stenosis in draining veins. Rapid flow in the feeding arteries may result in the development of arterial aneurysms, both in the same distribution as classic berry aneurysms (circle of Willis) and in feeding arteries (pedicle and nidal aneurysms) close to the malformation (Fig. 12-1). In addition, varices (venous aneurysms) can develop upstream to venous outflow stenosis and cause hemorrhage if they rupture (61). As a result of all these factors, AVMs are the vascular malformations that most commonly cause neurological defects other than seizures, despite the fact that they are not the most common form of vascular malformations.
Clinical Manifestations
Patients with AVMs usually present with seizures, recurrent headaches, progressive neurological deficits, hydrocephalus, or hemorrhage. Approximately 20% become symptomatic before the age of 20 years (43). The mortality associated with the initial rupture of an AVM is 10%, with morbidity between 30% and 50% (38,62). Morbidity and mortality increase with each subsequent hemorrhage.
AVMs are the cause of up to 40% of spontaneous intracranial hemorrhages (2,63,64), most of which occur in the cerebral parenchyma. However, superficial malformations can rupture into the subarachnoid space and deep malformations may cause intraventricular hemorrhage. Symptomatic vasospasm and rebleeding are relatively rare unless the source of hemorrhage is an associated aneurysm. The risk of rehemorrhage from an AVM has been estimated to be higher in children than adults (62). In children less than 15 years of age, AVMs are the most common cause of spontaneous intracranial hemorrhage and account for 20% of all strokes (2).
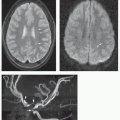
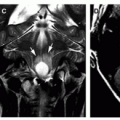
Figure 12-1 AVM with hemorrhage from a feeding artery aneurysm. A. Coronal reformatted CTA demonstrates dense vascular enhancement adjacent to the right lateral ventricular intraventricular hemorrhage. There is associated hydrocephalus. B. Axial T2-weighted image shows a circular structure within the lateral aspect of the intraventricular hemorrhage consistent with an aneurysm associated with a tangle of AVM nidus vessels in the corpus striatum just lateral to the right lateral ventricle. C. RAO image from a right internal carotid artery DSA shows the posterior corpus striatum AVM being fed by a medial lenticulostriate artery (recurrent artery of Heubner) that itself harbors the feeding artery aneurysm (white arrow) that hemorrhaged. D. The feeding artery aneurysm is more easily seen on a surface-rendered reformat of a 3D rotational angiogram of the right ICA.
Seizures occur in approximately 70% of patients with AVMs, with one-half of the seizures being generalized (65); most patients are well controlled with anticonvulsants. Seizures are most common in AVMs that are located in the cerebral cortex and have associated varices. Their cause is probably cortical injury and gliosis from previous hemorrhage (66) or venous ischemia (67,68).
Only gold members can continue reading. Log In or Register to continue
Nov 11, 2018 | Posted by drzezo in NEUROLOGICAL IMAGING | Comments Off on Anomalies of the Cerebral Vasculature: Diagnostic and Endovascular Considerations
 Introduction
Introduction Technical Considerations in Pediatric Neuroangiography and Intervention
Technical Considerations in Pediatric Neuroangiography and Intervention Intracerebral Hemorrhage in Children
Intracerebral Hemorrhage in Children Intracerebral Vascular Malformations
Intracerebral Vascular Malformations