- •
Before ordering any test, especially one associated with ionizing radiation, we must ensure the appropriateness of the study and that the potential benefits outweigh the risks.
- •
The use of dual isotope approaches (rest 201 Tl and stress 99m Tc agents) should be avoided because they are associated with the highest patient dose.
- •
Technetium-based radiopharmaceuticals should always be preferred for SPECT MPI.
- •
Whenever possible, PET MPI should be considered because it has the highest diagnostic accuracy and the lowest patient dose.
- •
The use of stress-only imaging protocols is the single most effective way to reduce patient dose. Implementation of stress-only imaging protocols requires careful patient selection, quality control, and experienced readers. Routine use of attenuation correction helps to reduce the number of patients in need of additional rest imaging.
- •
Previous data have demonstrated the equivalence of MPI with CZT cameras using a fraction of the radiotracer dose, which is generally administered with conventional SPECT camera.
- •
PET myocardial perfusion imaging with 82 Rb-chloride, 13 N-ammonia, or 15 O-water provides the most aggressive patient dose reduction approach for clinical nuclear cardiology.
- •
IQ•SPECT™ preserves both image quality and quantitative measurements with reduced acquisition time or administered dose in both phantom and clinical settings.
Introduction
Despite the undeniable patient benefits from medical imaging, there has been growing public concern about radiation exposure from medical imaging and its potential associated health risks. The latest report from the National Council on Radiation Protection and Measurements estimated that nuclear cardiology studies account for around 9% of the entire radiation burden from medical imaging to the U.S. population in 2016. The International Atomic Energy Agency (IAEA) has identified “8 best practices” that would help reduce the global radiation burden from cardiac radionuclide imaging ( Table 6.1 ). Likewise, the American Society of Nuclear Cardiology (ASNC) has set the goal of limiting the total radiation effective–dose of patients referred for single photon emission computed tomography (SPECT) or positron emission tomography (PET) myocardial perfusion imaging (MPI) to less than or equal to 9 mSv. Nevertheless, recent studies have reported that most of the dose-reduction approaches and best practices, especially adequate radiopharmaceutical and protocol selection, are still underutilized in clinical practice, with most SPECT MPI studies still exceeding the 9 mSv benchmark.
| Best Practices | |
|---|---|
| 1. Appropriately use radionuclide imaging | Ensure appropriate indication for the study. |
| 2. Avoid 201 Tl imaging | 201 Tl is associated with considerably higher radiation doses to patients. When needed, inject no more than 3.5 mCi (129 MBq). |
| 3. Avoid dual isotope (rest 201 Tl – stress 99m Tc) | Dual isotope MPI is associated with the highest radiation dose of any protocol. |
| 4. Avoid too much 99m Tc | For single-day protocols, keep the total 99m Tc dose <35 mCi (1295 MBq). |
| 5. Perform stress-only imaging | When clinically appropriate, stress-only imaging can lead to a considerably lower radiation dose. |
| 6. Use camera-based dose-reduction strategies | These include: (i) attenuation correction, (ii) imaging patients in multiple positions (e.g., supine and prone), (iii) software (e.g., incorporating iterative reconstruction, resolution recovery, and noise reduction), and (iv) high-technology hardware (e.g., solid-state SPECT camera, cardiac-focused collimator). Each of these approaches reduces the radiation dose needed or facilitates performance of stress-only imaging. |
| 7. Weight-based dosing for 99m Tc | Tailoring the administered activity to the patient size offers an opportunity to reduce radiation dose. |
| 8. Use PET imaging | When available and appropriate, the use of PET imaging helps reduce radiation dose. |
This chapter will review new technology and strategies that are available to reduce radiation exposure to patients without affecting image quality or diagnostic information from nuclear cardiology studies.
New technology to limit patient dose
The new technology includes innovations in both hardware and image processing software. The following sections contain brief descriptions of individual hardware and software advances. Nevertheless, it must be emphasized that hardware and software solutions are almost always implemented together. These technological advances in both hardware design and reconstruction software for MPI afford the opportunity to reduce health risk by lowering patient dose, increasing patient comfort by reducing the scan time, or both. Please refer to Chapters 1 and 2 for a more detailed discussion of these new technological advances.
Hardware
Collimator redesign
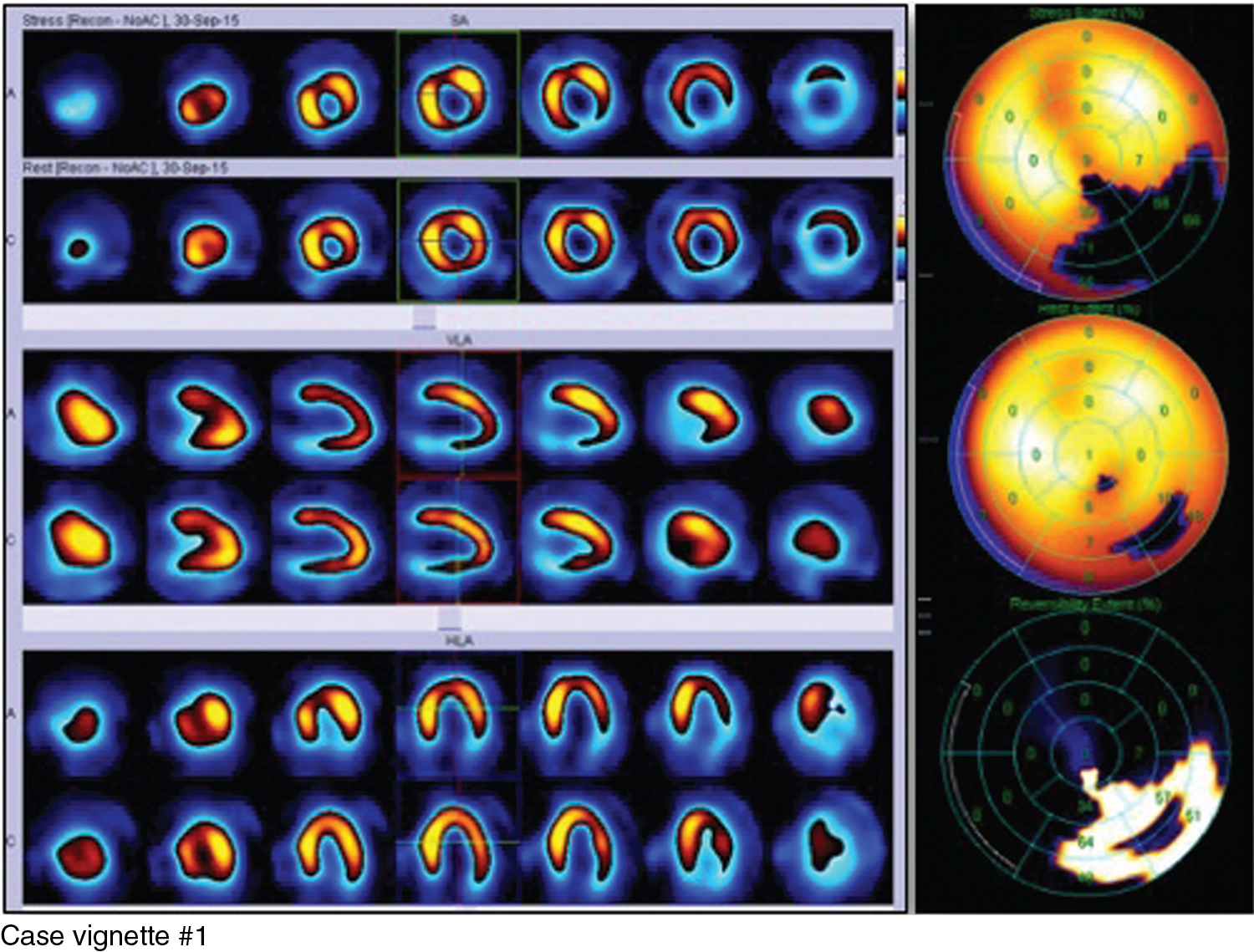
Case vignette #1
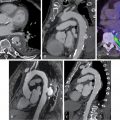
A 74-year-old woman presents with a history of hypertension, hypercholesterolemia, and coronary artery disease (CAD) with prior revascularization by percutaneous coronary intervention (PCI) of the diagonal, left circumflex, and right coronary arteries, and is evaluated for exertional dyspnea. She underwent dipyridamole-stress and rest myocardial perfusion scintigraphy using IQ•SPECT™ technology. A 12-minute stress scan was obtained 35 minutes after the intravenous (IV) injection of 4.8 mCi (180 MBq) 99m technetium (Tc)-tetrofosmin. This was followed by a 15-minute rest scan after the IV injection of 13 mCi (470 MBq) 99m Tc-tetrofosmin. The myocardial perfusion SPECT images demonstrate a medium-sized perfusion defect of severe intensity throughout the inferior and inferolateral walls, showing significant but not complete reversibility consistent with significant stress-induced ischemia ( Fig. 6.1 ). The electrocardiogram (ECG)-gated images showed a normal left ventricular ejection fraction (LVEF) at stress (65%) and rest (67%). The estimated whole-body effective dose was 4.6 mSv.
The prototype in this category is the IQ•SPECT™ technology (Siemens Medical Solutions USA, Inc.). It consists of a multifocal collimator called SmartZoom for heart-centered collimation, together with cardio centric image acquisition and dedicated reconstruction software, which, when combined, allows for sensitivity fourfold higher than conventional low-energy, high-resolution (LEHR) collimators. , One advantage of this multifocal collimator is that it can be applied to conventional multipurpose gamma cameras. As in the case of conventional MPI, IQ•SPECT™ technology is subject to photon attenuation artifacts that may degrade image quality and impair the diagnostic accuracy. In particular, because of the collimator’s intrinsic geometry, the photon trajectories of voxels are characteristically different than with conventional LEHR collimators, typically resulting in relatively more counts in the left ventricular (LV) apex and fewer counts in the inferolateral regions, which may impair image interpretation. Consistent data, however, demonstrate that those artifacts can be managed appropriately by means of either CT-based attenuation correction or, in its absence, with combined supine and prone acquisitions that may homogenize to some extent LV counts and significantly reduce false readings. Accordingly, validation studies have demonstrated that IQ•SPECT™ effectively preserves both image quality and quantitative measurements with reduced acquisition time or administered dose in both phantom and clinical settings with a comparable assessment of both LV functional and perfusion information. An important aspect for the correct data interpretation is the need for specific normalcy databases for the different radiotracers’ distribution, particularly if noncorrected or supine/prone images are evaluated.
Solid state detector cameras
Case vignette #2
A 58-year-old man with a history of hypertension, hypercholesterolemia, and active cigarette smoking is referred for evaluation for atypical angina and exertional dyspnea. He underwent a stress-rest SPECT myocardial perfusion study using a solid-state detector camera. He exercised for 7 minutes of a modified Bruce protocol, achieving 87% of the age-predicted maximal heart rate. The symptomatic response to exercise was abnormal because of dyspnea. The ECG response to exercise indicated no significant ST-T changes. Stress images were obtained for 7 minutes beginning 15 minutes after the IV injection of 4.2 mCi (155 MBq) 99m Tc-tetrofosmin. Sixty minutes later, rest images were obtained for 6 minutes beginning 30 minutes after the IV injection of 8.4 mCi (310 MBq) 99m Tc-tetrofosmin. The myocardial perfusion SPECT images showed small areas of moderate stress-induced ischemia in the apical and mid anterolateral as well as in the basal inferior and inferoseptal walls ( Fig. 6.2 ). The ECG-gated images showed a normal LVEF at stress and rest (58% and 57%, respectively). Subsequent invasive coronary angiography demonstrated significant stenoses in the left anterior descending and right coronary arteries, both of which were stented. The estimated whole-body effective dose was 3.3 mSv.