Fig. 8.1
Illustration showing the relevant anatomy of the atlanto-occipital and atlanto-axial joints
The C2 nerve root, dorsal root ganglion, and its surrounding dural sleeve cross the posterior aspect of the middle of the joint. Therefore, during AAJ injection, the needle should be directed towards the junction of the middle and lateral thirds of the posterior aspect of the joint. This will avoid injury to the C2 nerve root medially or the vertebral artery laterally (Fig. 8.1) [1, 7]. Conversely, the AOJ should be accessed posteriorly from the most superior lateral aspect to avoid injuring the vertebral artery medially.
Technique of AAJ Injections
With the patient placed in the prone position and a pillow under the chest to allow for slight neck flexion, the fluoroscopy C-arm is brought to the head of the table in an anteroposterior direction. Under fluoroscopic guidance, the C-arm is rotated in a cephalad-caudad direction to better visualize the lateral AAJ. The needle insertion site is marked on the skin overlying the lateral thirds of the AAJ. The skin is prepped and draped in the usual sterile fashion, and a skin wheel is raised with local anaesthetic at the insertion site. Then a 22–25-G 3½ inches blunt needle is advanced towards the posterolateral aspect of the inferior margin of the inferior articular process of the atlas (C1). This will avoid contact with the C2 nerve root and dorsal ganglion, which crosses the posterior aspect of the middle of the joint. It is “better” to seek and touch the bone to safely establish the correct depth. At this point, a lateral view is obtained. The needle is withdrawn slightly, directed towards the posterolateral aspect of the lateral atlanto-axial joint, and advanced for couple of millimetres. Usually a distinctive pop is felt signalling entering the joint cavity. Careful attention should be paid to avoid the vertebral artery that lies laterally to the lateral AAJ as it courses through the C1 and C2 foramina. After careful negative aspiration for blood or cerebrospinal fluid, 0.1–0.2 ml of water-soluble nonionic contrast agent is injected to verify intra-articular placement of the tip of the needle.
Injection of the contrast agent is done under direct real-time fluoroscopy to check for inadvertent intra-arterial injection which is manifest by rapid clearance of the contrast agent. Anteroposterior and lateral views are obtained to insure that the contrast agent remained confined to the joint cavity without escape to the surrounding structures, especially the epidural space, or posteriorly to the C2 ganglion which will adversely affect the specificity of the block (Figs. 8.2 and 8.3). The anteroposterior view usually demonstrates the bilateral concavity of the joint with the contrast material inside the joint space (Fig. 8.2), and sometimes it shows that the lateral AAJ space communicates with that of the median atlanto-axial joint (Fig. 8.4) and the contralateral AAJ (Fig. 8.5). After careful negative aspiration, 1.0 ml of a mixture of bupivacaine 0.5 % and 10 mg of triamcinolone is injected.
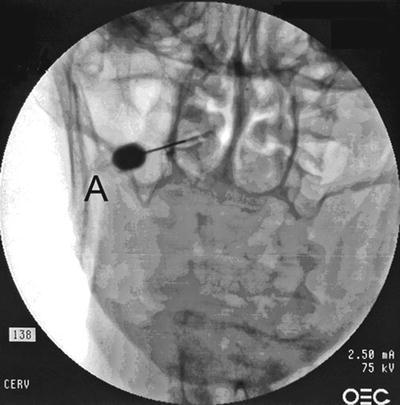
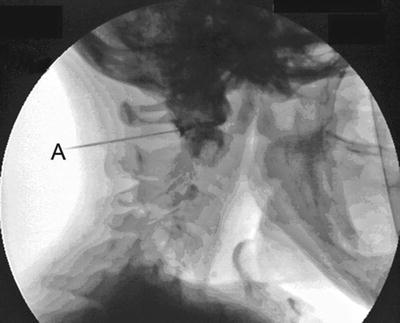


Fig. 8.2
Lateral atlanto-axial joint (AAJ) injection: AP view showing the needle (A) targeting the lateral third of the joint, and the contrast is contained within the joint space (Reproduced with permission from Ohio Pain and Headache Institute)
Fig. 8.3
Lateral atlanto-axial joint (AAJ) injection: lateral view showing the needle (A) and the contrast contained within the joint space (Reproduced with permission from Ohio Pain and Headache Institute)
Fig. 8.4
Lateral atlanto-axial joint (AAJ) injection: A lateral atlanto-axial joint (AAJ). B contrast agent within the AAJ. C contrast spreading to the median atlanto-axial joint (Reproduced with permission from Ohio Pain and Headache Institute)
Fig. 8.5
Lateral atlanto-axial joint (AAJ) injection: Needle inside the left AAJ with the contrast spreading to the right AAJ (arrow) (Reproduced with permission from Ohio Pain and Headache Institute)
Related posts:
 Transforaminal Epidural Steroid Injections
Transforaminal Epidural Steroid Injections
 Stellate Ganglion Blockade
Stellate Ganglion Blockade
 Clinical Applications of Neuromodulation: Section on Angina and Peripheral Vascular Disease
Clinical Applications of Neuromodulation: Section on Angina and Peripheral Vascular Disease
 Suprascapular Nerve Block
Suprascapular Nerve Block
 Spinal Targets for Interventional Pain Management
Spinal Targets for Interventional Pain Management
 Stimulation of the Peripheral Nerve and Peripheral Nerve Field
Stimulation of the Peripheral Nerve and Peripheral Nerve Field
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


