CHAPTER 4
Atrial Septal Defects
Definition
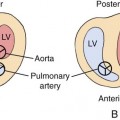
ASDs are classified according to their embryogenesis, their location relative to the fossa ovalis, and their size. There are four types of ASDs, listed here in order of frequency, with ostium secundum ASDs making up approximately 80% of cases (Fig. 4–1):
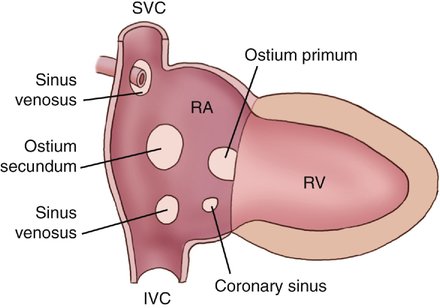
1. Sinus venosus ASDs of the superior vena cava (SVC) type are located just inferior to the orifice of the SVC in the right atrium so that the SVC overrides the ASD, providing blood to both atria. Sinus venosus ASDs of the SVC type closely approximate the site where the right pulmonary veins enter the left atrium, allowing anomalous pulmonary venous drainage through the ASD. This type of ASD is present in partial anomalous pulmonary venous return to the right atrium.1
2. Sinus venosus ASDs of the inferior vena cava type are located in the atrial septum, adjacent to the orifice of the inferior vena cava in the right atrium.
The common atrium, the most severe form of ASD, is defined as an ASD involving >50% of the interatrial septum. Common atrium is rarely an isolated anomaly.1
Embryology
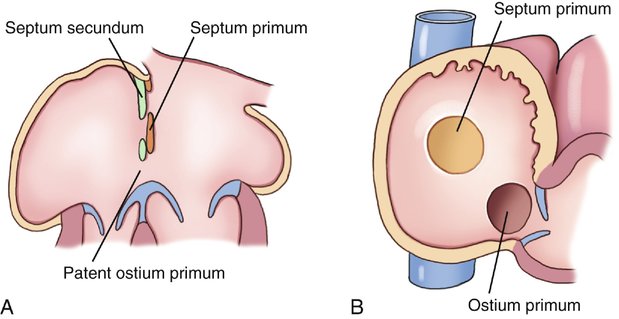
Between the fourth and sixth weeks of gestation, the primitive atrium is divided into right and left halves by a complex series of events. Throughout this process, some degree of interatrial blood flow is maintained. The septum primum, a thin, mobile, crescent-shaped membrane, develops along the cephalad portion of the atrium and grows caudally toward the endocardial cushions (Fig. 4–2, A). The space between the septum primum and the endocardial cushions, termed the ostium primum, is eventually obliterated when the septum primum fuses with the endocardial cushion (Fig. 4–2, B to D). Before complete fusion, however, multiple small fenestrations develop in the septum primum, coalescing to form the ostium secundum (Fig. 4–2, B to D), maintaining free blood flow from the right to the left primitive atrium.
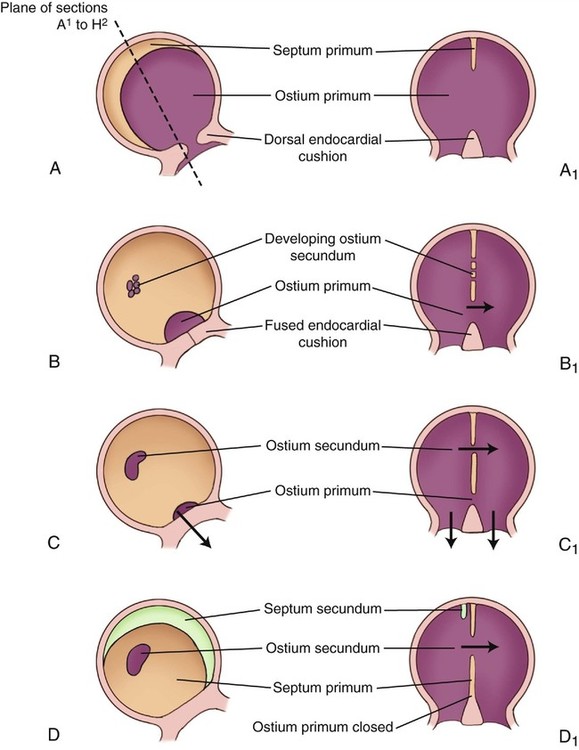
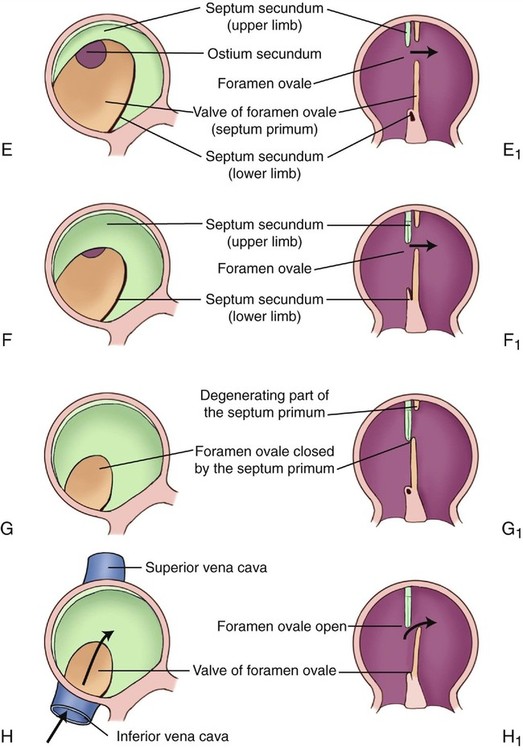
A second crescent-shaped membrane, the septum secundum, subsequently develops just to the right of the septum primum (Fig. 4–2, D to F). The thick muscular septum secundum is formed from invagination of the roof of the primitive common atrium. As this membrane grows toward the endocardial cushions, it covers the ostium secundum (Fig. 4–2, E and F). Its crescent-shaped lower border never fuses entirely with the endocardial cushion, leaving an opening that represents the foramen ovale (Fig. 4–2, E and F). The upper portion of the septum primum is gradually resorbed, and the remaining lower portion becomes the valve of the foramen ovale or foraminal flap (Fig. 4–2, G and H).
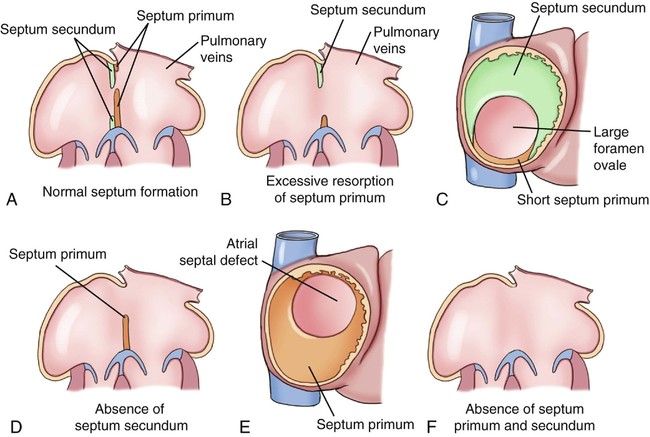
The most common type of ASD, the ostium secundum defect, is caused by a shortened valve of the foramen ovale (foraminal flap) resulting from excessive resorption of the septum primum or to deficient growth of the septum secundum (Fig. 4–3).
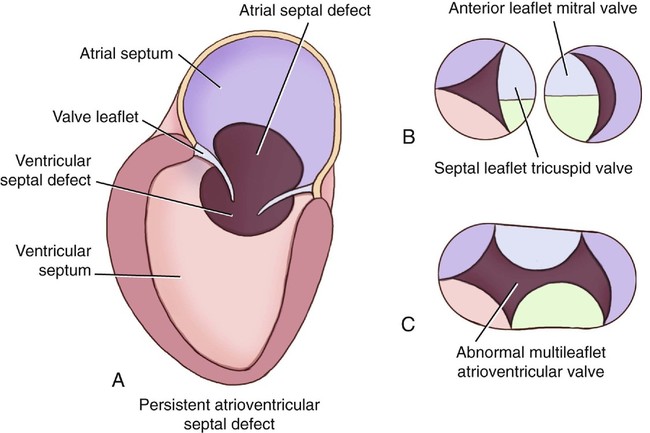
The ostium primum ASD occurs when the lower portion of the atrial septum, which is partially formed from the endocardial cushions, is deficient and fuses incompletely with the endocardial cushions (Fig. 4–4). This defect can occur in isolation but is usually part of the more complex atrioventricular septal defect, also referred to as an endocardial cushion defect or an atrioventricular canal defect, in which a single large abnormal atrioventricular valve separates the atria and ventricles in the presence of a large ASD and ventricular septal defect (VSD) (Fig. 4–5).
The sinus venosus ASD occurs during embryogenesis when the right horn of the sinus venosus, which normally encompasses the orifice of the SVC and the inferior vena cava, develops abnormally, leaving an opening in the atrial septum near one of these orifices (see Fig. 4–1).
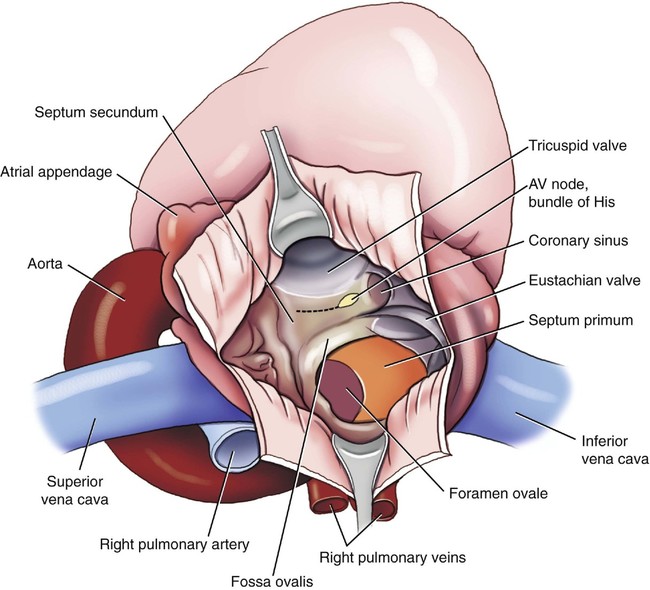
The coronary sinus ASD occurs when improper development of the coronary sinus allows it to communicate directly with the left atrium through a defect in the wall of its distal extremity, leaving an open channel from the right atrium through the coronary sinus and into the left atrium (see Fig. 4–1). Even in the absence of structural defects, the anatomy of the normal neonatal atrial septum is complex (Fig. 4–6).
Occurrence Rate
ASDs occur in 1 in 1500 live births,2,3 and they comprise approximately 6.7% of congenital heart disease in live-born infants.4 Overall, ASDs are twice as common in female infants than in male infants.5,6
Ostium secundum defects account for more than 80% of all ASDs5 and occur twice as often in female patients.7 Sinus venosus defects account for 5% to 10% of all ASDs and occur with equal frequency in male and female patients.8 Coronary sinus defects are rare. Various combinations of these types of ASD can occur together.
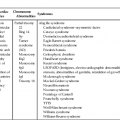
Rarely, ostium secundum ASDs are familial and may occur through multiple generations.9–12 Perhaps the best known example of familial inheritance of ASD is the Holt-Oram syndrome.13 This disorder is characterized by an autosomal dominant pattern of inheritance with a penetrance of nearly 100%. In addition to a septum secundum ASD, patients have congenital deformities of the upper limbs (most commonly with absent or hypoplastic radii) and cardiac rhythm abnormalities such as a right bundle branch block or first-degree atrioventricular block. Approximately 40% of these cases represent new mutations. The remainder are inherited from a parent.
A second example of familial inheritance of ASD (also ostium secundum type) is the syndrome of familial ASD with prolonged atrioventricular conduction.14

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


