Fig. 32.1
Sagittal T2 STIR MRI shows significant signal alteration involving the first lumbar vertebral body, with epidural pathologic tissue and slight dural sac compression
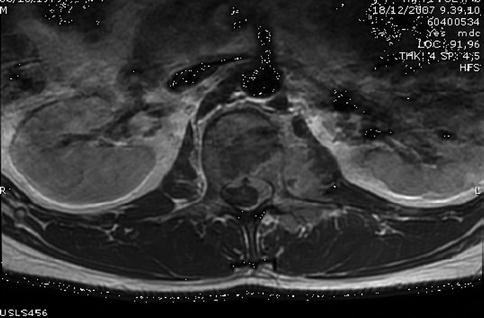
Fig. 32.2
Axial T1 MRI sequence after contrast administration shows intense enhancement of the vertebral body and epidural tissue
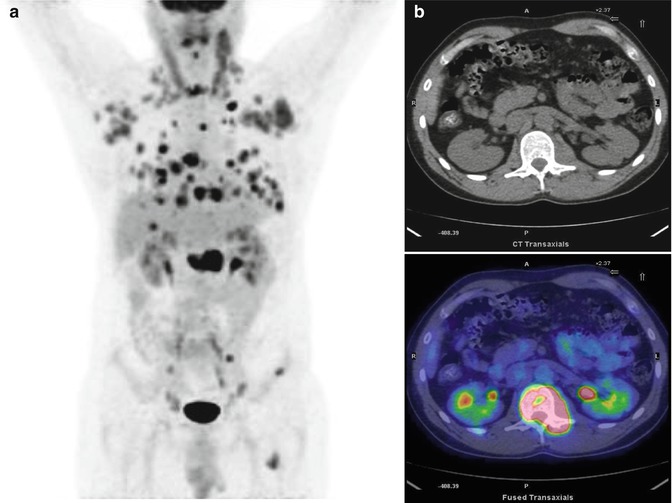
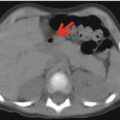
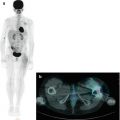
Fig. 32.3
Maximum intensity projection (a) shows intense FDG uptake in the vertebrae, ribs, sacrum, left femor, liver, and both lungs. Further uptake was detected in multiple lymph nodes distributed at cervical, thoracic, and abdominal stations. Axial CT and PET/CT fusion images (b) show intense FDG uptake in the first lumbar vertebral body
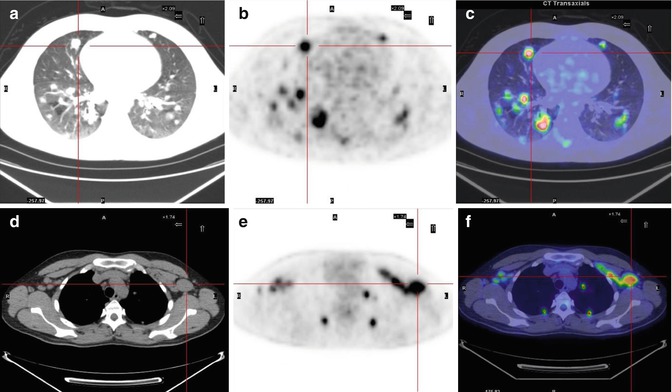
Fig. 32.4
(a–c) Axial CT with lung window (a), PET (b), and PET/CT fusion (c) images show multiple uptake in both lungs. (d–f) Axial CT with mediastinal window (d), PET (e), and PET/CT fusion (f) images show tracer accumulation in the axillary lymph nodes

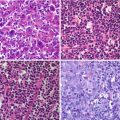
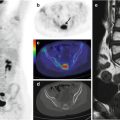
Fig. 32.5




Axial CT (a), PET (b) and PET/CT fusion (c) images depict a FDG-avid focus in the left iliac bone. A PET-guided bone marrow biopsy was performed at the site of tracer uptake in the left iliac bone. Based on the findings, the definitive diagnosis was non-Hodgkin’s lymphoma
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
