High risk: Midesophageal stricture, ulcer, reticular mucosa
Moderate risk: Distal peptic stricture and reflux esophagitis
Low risk: If none of above findings are present
• Diagnosis: Endoscopy with biopsy
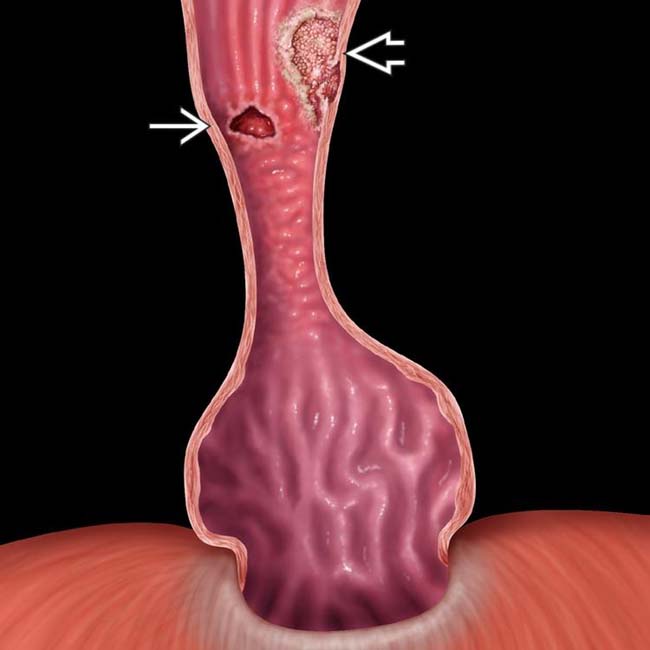
(Left) Graphic shows a type 1 hiatal hernia, distal esophageal stricture, and nodular mucosal surface. Note the discrete ulcer and an adenocarcinoma represented by a raised sessile lesion with an irregular surface.
(Right) 2 views from an esophagram show a mid esophageal stricture and ulcer in a patient with a small hernia and reflux.
(Left) Endoscopic image shows a large ulcer with the velvet texture of Barrett mucosa and stricture. Normal esophageal mucosa has a shiny, smooth, pink surface.
(Right) Two views from an esophagram show a polypoid mass that represents an adenocarcinoma arising in Barrett mucosa.
TERMINOLOGY
Definitions
• Metaplasia of distal esophageal squamous epithelium to columnar epithelium
IMAGING
General Features
• Best diagnostic clue
Mid esophageal stricture with hiatal hernia and reflux is essentially pathognomonic
• Other general features
Acquired condition due to reflux esophagitis
Premalignant condition associated with increased risk of esophageal adenocarcinoma
– Risk: 30-40x higher than in general population
– 90-100% of adenocarcinomas arise from Barrett mucosa
Radiographic Findings
• Double contrast esophagography is imaging of choice
• Classified into 2 types based on endoscopy and histopathologic findings
Long segment: Columnar epithelium > 3 cm above gastroesophageal (GE) junction
– Due to more severe reflux disease
– Hiatal hernia in almost all patients
Only gold members can continue reading. Log In or Register to continue









 and an adenocarcinoma
and an adenocarcinoma  represented by a raised sessile lesion with an irregular surface.
represented by a raised sessile lesion with an irregular surface.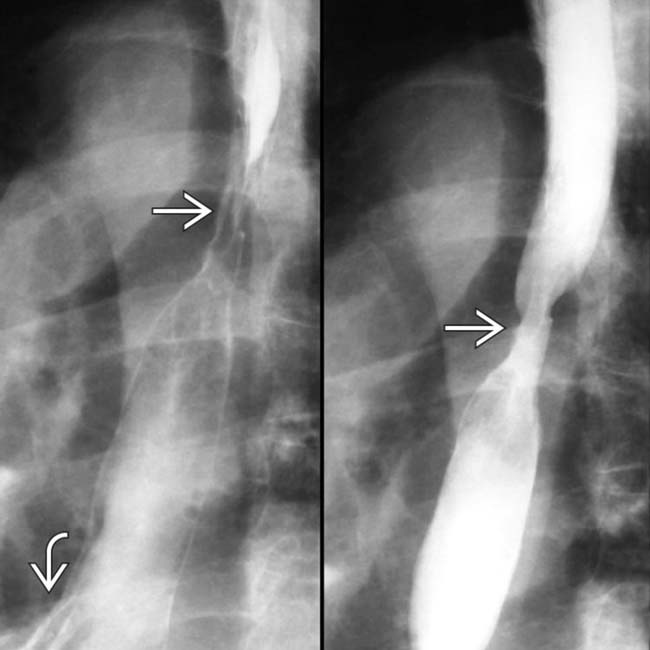
 and ulcer in a patient with a small hernia
and ulcer in a patient with a small hernia  and reflux.
and reflux.
 with the velvet texture of Barrett mucosa and stricture. Normal esophageal mucosa has a shiny, smooth, pink surface.
with the velvet texture of Barrett mucosa and stricture. Normal esophageal mucosa has a shiny, smooth, pink surface.
 that represents an adenocarcinoma arising in Barrett mucosa.
that represents an adenocarcinoma arising in Barrett mucosa.


 Long segment: Columnar epithelium > 3 cm above gastroesophageal (GE) junction
Long segment: Columnar epithelium > 3 cm above gastroesophageal (GE) junction



