• Traumatic bile leaks due to blunt or penetrating trauma can occur but are relatively uncommon
CLINICAL ISSUES
• ERCP with sphincterotomy and plastic stent placement (to decrease biliary pressure and control leak) is effective in majority (> 90%) of cases
• Percutaneous drainage of collection (often under image guidance) if biloma is large, infected, or increasing in size
• Biloma associated with transection of extrahepatic duct may require hepaticojejunostomy
(Left) Axial CECT in a patient who had recently undergone partial hepatectomy demonstrates development of a biloma in the surgical bed.
(Right) Frontal ERCP image in the same patient demonstrates active extravasation of contrast into the biloma from the right hepatic lobe bile duct distribution. Unlike other imaging modalities, ERCP can definitively identify an active bile leak and confirm that a fluid collection represents a biloma.
(Left) Axial CECT in a patient with fever and abdominal pain 21 days after a laparoscopic posterior segment wedge resection of a small hyalinized hemangioma shows a central right lobe biloma and surrounding devascularized, infarcted liver .
(Right) ERCP of the same patient shows a bile leak with spillage of contrast into the biloma, and an appropriately positioned drain . The biloma completely resolved after percutaneous drainage and biliary stent placement.
TERMINOLOGY
Definitions
• Loculated collection of bile within abdomen resulting from bile leak
IMAGING
General Features
• Best diagnostic clue
Loculated fluid collection of simple fluid attenuation in close proximity to liver or biliary tree
• Location
Either intrahepatic or extrahepatic
– Most commonly perihepatic (gallbladder fossa, Morison pouch) and subphrenic
• Size
2-20 cm
• Morphology
Usually encapsulated and rounded
May be lentiform if subcapsular
Imaging Recommendations
• Best imaging tool
CECT or Tc-99m IDA
• Protocol advice
Biliary scintigraphy: Sequential 1-minute acquisition for 60 minutes; static imaging at 2-4 hours and at 24 hours (if required)
Radiographic Findings
• ERCP can delineate site of leakage and presence of aberrant ducts that might change treatment approach
May identify site of leak either within intrahepatic ducts or within extrahepatic bile ducts (e.g., cystic duct, common hepatic duct, or aberrant right hepatic duct)
Can delineate injury to aberrant duct (e.g., aberrant right hepatic duct) that may change management
CT Findings
• Water-attenuation fluid collection within or adjacent to liver with exertion of mass effect on adjacent structures
Usually simple in appearance, but may rarely have internal debris, blood products, etc.
Usually no identifiable capsule or peripheral enhancement
• Subcapsular or intrahepatic biloma may result in adjacent transient hepatic attenuation difference (THAD) during arterial phase imaging (secondary to mass effect and diminished portal venous flow)
MR Findings
• Typically well-defined fluid collections, which are T2WI hyperintense and T1WI hypointense
No internal/peripheral enhancement or capsule
• MRCP delineates relationship of biloma with adjacent biliary tree and anomalies in bile duct anatomy
Cannot definitively identify site of bile leak or differentiate biloma from other fluid collections
• Hepatobiliary contrast agents (e.g., Eovist) are excreted into biliary tree and may identify site of bile leak
Active extravasation visualized in hepatobiliary phase
– Delayed images helpful in patients with biliary dilatation or impaired hepatic function to increase sensitivity
High reported sensitivities for bile leaks (∼ 100%)
Technique limited in patients with impaired liver function who may not demonstrate adequate excretion of contrast into biliary tree
Ultrasonographic Findings
• Usually simple intrahepatic/perihepatic fluid collection
• May have low-level echoes due to hemorrhage/infection
Nuclear Medicine Findings
• Hepatobiliary scintigraphy
Focal accumulation of radiotracer outside biliary tree/bowel
Only gold members can continue reading. Log In or Register to continue

 Hepatobiliary contrast agents (e.g., Eovist) are excreted into biliary tree and may identify site of bile leak in hepatobiliary phase
Hepatobiliary contrast agents (e.g., Eovist) are excreted into biliary tree and may identify site of bile leak in hepatobiliary phase

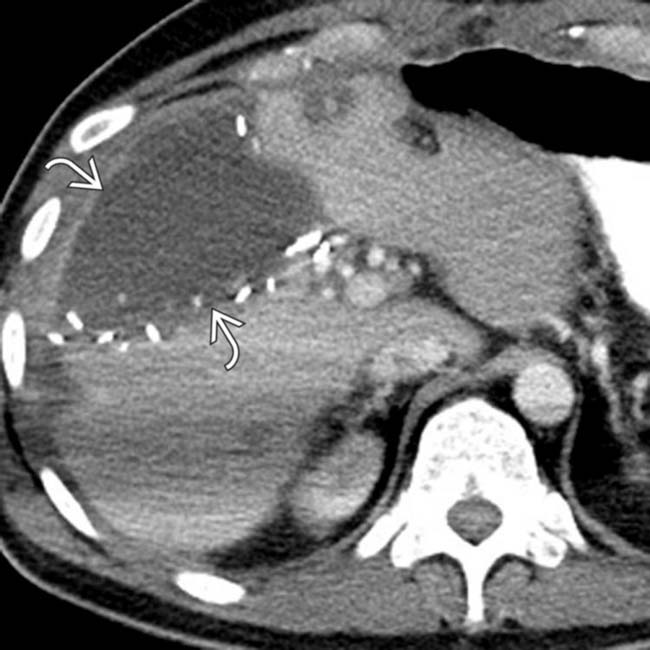
 in the surgical bed.
in the surgical bed.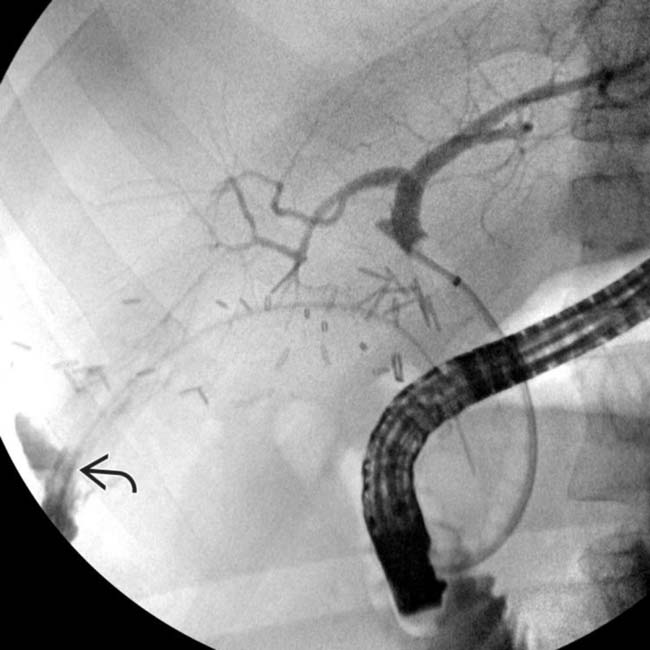
 of contrast into the biloma from the right hepatic lobe bile duct distribution. Unlike other imaging modalities, ERCP can definitively identify an active bile leak and confirm that a fluid collection represents a biloma.
of contrast into the biloma from the right hepatic lobe bile duct distribution. Unlike other imaging modalities, ERCP can definitively identify an active bile leak and confirm that a fluid collection represents a biloma.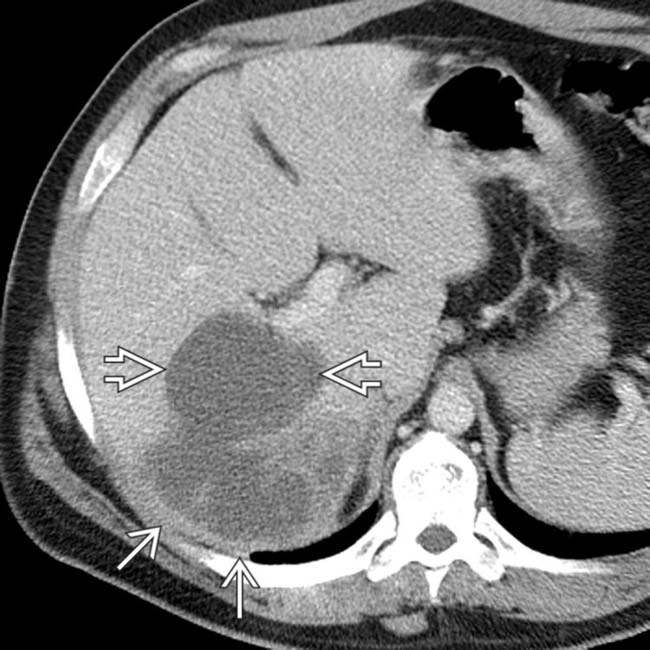
 and surrounding devascularized, infarcted liver
and surrounding devascularized, infarcted liver  .
.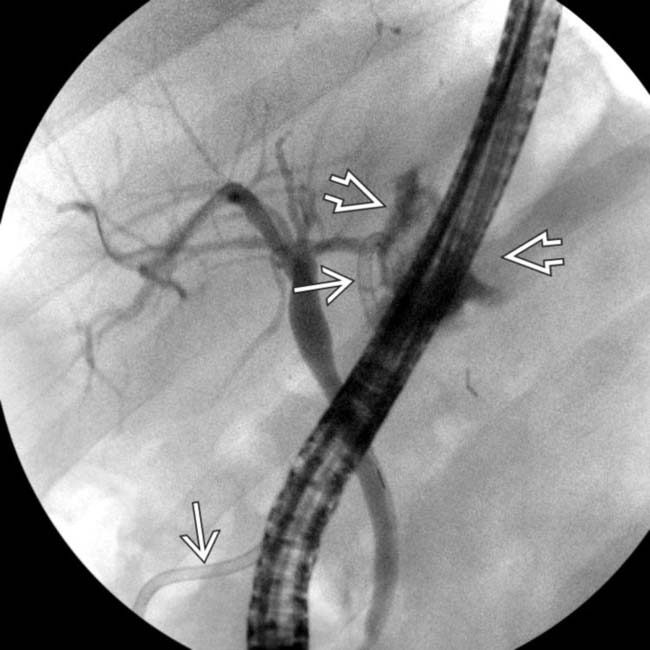
 into the biloma, and an appropriately positioned drain
into the biloma, and an appropriately positioned drain  . The biloma completely resolved after percutaneous drainage and biliary stent placement.
. The biloma completely resolved after percutaneous drainage and biliary stent placement.





















